4 Practical Tips for Hashimoto’s Thyroiditis & Hypothyroid Symptoms
Written by ![]() Dr. Michael Ruscio, DC on
June 6, 2018
Dr. Michael Ruscio, DC on
June 6, 2018
Hypothyroidism and thyroid autoimmunity are shrouded in fear and confusion, but it doesn’t have to be this way. There are simple, evidence-based and practical strategies that can help you determine if you actually have hypothyroid or thyroid autoimmunity. It’s important to know if you have either of these, so you can act. It’s equally as important to know if you do not, so you can prevent unnecessary fear, testing and treatment.
What are healthy levels of Thyroid antibodies?
Thyroperoxidase antibodies (aka TPO ab)
- Between 100-300 (roughly) is considered a clinical win
- Normal reference range is < 35 UI
- The higher the levels the greater the risk of developing true hypothyroidism in the future
Thyroglobulin antibodies (aka TG ab)
- Less than 10 times the reference range
- Normal reference range is equal/below 1 IU/mL
- Less data available here, not as predictive, worry less about this value
Conclusion
- There is a relationship between antibodies and risk of hypothyroidism and depressed well-being
- Don’t be too concerned with slightly elevated antibodies if you eat well and feel healthy
- To summarize the studies below (and in the audio), researchers found that TPO-Abs below 500 IU/mL posed a minimal risk for being or becoming hypothyroid, while TPO-Abs above 500 IU/mL posed a moderate risk of developing hypothyroidism. These studies further support that TPO-Abs <500 could be considered a clinical win.
Hypothyroid versus Hashimoto’s
- Hashimoto’s means you have elevated antibodies (most commonly TPO and TG) and/or ultrasound changes to thyroid gland (hypoechogenicity)
- A process wherein immune cells damage your thyroid gland
- One can have Hashimoto’s and have normal thyroid function and be perfectly healthy, however, highly-elevated antibodies (>500 for TPO) moderately increases risk of developing hypothyroidism in the future
- Hypothyroid means you have high TSH paired with low free T4, according to conventional ranges
- Most cases of hypothyroidism require medication to restore normal blood levels of thyroid hormone
Symptoms that correlate with hypothyroidism
- In this study 13 symptoms were statistically overrepresented in hypothyroidism:
- globus sensation, difficulty swallowing, anterior neck pain
- wheezing, shortness of breath, palpitations
- constipation, hair loss, dry skin
- restlessness, mood lability, tiredness, and vertigo
- Reporting 3 or more of these symptoms was significantly associated with autoimmune hypothyroid
- If fatigue is not present than hypothyroid is unlikely
- If dry skin is not present than hypothyroid is unlikely
True hypothyroid versus “functionally low thyroid”
- One is a disease, one is not
- One may require long-term medication, one does not
What to do?
Identify if you are hypothyroid.
- If yes, start on medication
- A T4/T3 combo may work better for some, not for all
- Sensitive/reactive patients may do better on a cleaner form, Nature-Thyroid
- If no
- Look to other system of body as cause of symptoms
Identify if you have Hashimoto’s
- Over >300-500 TPO – take action to improve antibodies
- Under <300-500 – no action required. Or, consider action if none has been taken previously.
- Diet: Lower carb, gluten reduced diet
- Supplementation: Vitamin D, Selenium, Mg, CoQ10,
- Improve gut health
Optimizing gut health can lead to:
- Reduction of medication
- Improvement of autoimmunity
- Improvement of non-responsive hypothyroid symptoms
In This Episode
Episode Intro … 00:00:40
Healthy Levels of Thyroid Antibodies … 00:02:47
Conclusion of Studies … 00:03:50
Hypothyroid Versus Hashimoto’s … 00:11:39
Hypothyroidism Symptoms … 00:13:30
True Hypothyroid Vs Functionally Low Thyroid … 00:16:30
What To Do … 00:20:10
Selenium … 00:27:50
Case Study Hypothyroid Hashimoto’s … 00:31:09
Case Study Thyroid Nodule … 00:31:48
Case Study Hashimoto’s … 00:32:48
Episode Wrap-Up … 00:34:45
Subscribe for future episodes



Download this Episode (right click link and ‘Save As’)
Episode Intro
Dr. Michael Ruscio, DC: Hey, everyone. This is Dr. Ruscio. And today I have, I guess what you could call a special treat where we will go through a presentation I recently gave. The presentation is entitled “Thyroid Autoimmunity: What are Healthy Levels for Thyroid Antibodies?” And I put together this presentation to help provide people with a little bit more clarity regarding thyroid antibodies, what they mean, what their clinical significance is. It’s important to understand this issue to know when to act.
However, it may be equally as important to understand when not to act and know this so as to dissipate any unnecessary fear which can certainly detract from one’s health. So having a reasonable, practical, accurate, and clinically meaningful understanding of thyroid antibodies, what they mean, and what you should do about a given level of antibody that you may have. So let’s jump in.
The outline. I’m sorry. Let me make one remark here. The video for this is available on the website just in case you missed that in the intro. So first, we’ll discuss what are healthy levels of thyroid antibodies. Second, what hypothyroid versus Hashimoto’s, what they are and how we identify those. Third, true hypothyroid versus functionally low thyroid. This is a key distinction. And fourth, what to do.
Also, let me mention that this is not meant to be an exhaustive review of the issue. This presentation will take about 20 minutes. I can give you a lot of value in that 20 minutes, but it’s not going to cover every nuance. But this will give you what I think will be the nuts and bolts of a very solid approach to thyroid. Ok.
Healthy Levels of Thyroid Antibodies
What are healthy levels of thyroid antibodies? Specifically, let’s cover the thyroperoxidase antibody or TPO. So in my opinion, roughly between 100-300 can be considered a clinical win. The normal reference range is usually below 35. The higher the levels the greater the risk of developing true hypothyroidism in the future. And there’s also the risk of impaired sense of well-being.
Thyroglobulin antibodies, aka TG antibodies. Less than 10 times the reference range is what I consider to be normal. The normal reference range is equal to or below 1.0. There is much less data here. And therefore, it is not as predictive. So don’t worry that much about this value. Worry more so about the TPO.
Conclusion of Studies
I’ll start with the conclusion, and then we will work to support that conclusion. There is a relationship between antibodies and, one, risk of hypothyroidism and, two, a depressed sense of well-being. However, this appears only to apply when significantly positive. So low-level positive findings may not pose a risk, and we’ll detail that more in a moment. So don’t freak out about mildly elevated antibodies, especially if you are already eating well and feeling healthy.
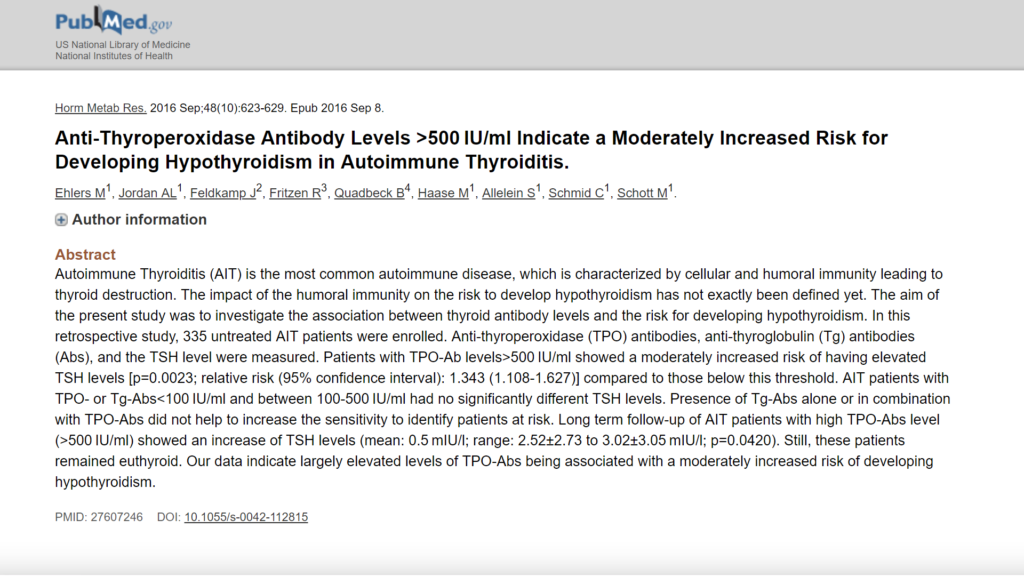
Let’s go into the evidence now that supports my position. From the Journal of Hormone and Metabolic Research. (1) Essentially, these researchers found that a TPO below 500 posed a minimal risk for being or becoming hypothyroid, while TPO antibodies above 500 posed a moderate risk of developing hypothyroidism. And again, I’m using very specific language here because the details here do matter. A minimal risk and a moderate risk. This is important. Oftentimes, people will only tell you if you have antibodies you will have hypothyroidism. It’s not really true to say that globally and definitively.
What’s more true is to be accurate in discerning with how we’re using our language and to understand that antibodies—at least according to the best evidence that we have to date. This may change in the future. But according to the best evidence we have to date, being above 500 poses a moderate risk and being a minimal risk when below 500. So it’s important to understand that. This suggests that a TPO antibody below 500 might be considered a clinical win and associated with minimal risk, as these researchers found. Translation: Otherwise healthy patients with TPO antibodies below 500 may not require further treatment to drive down their antibodies.
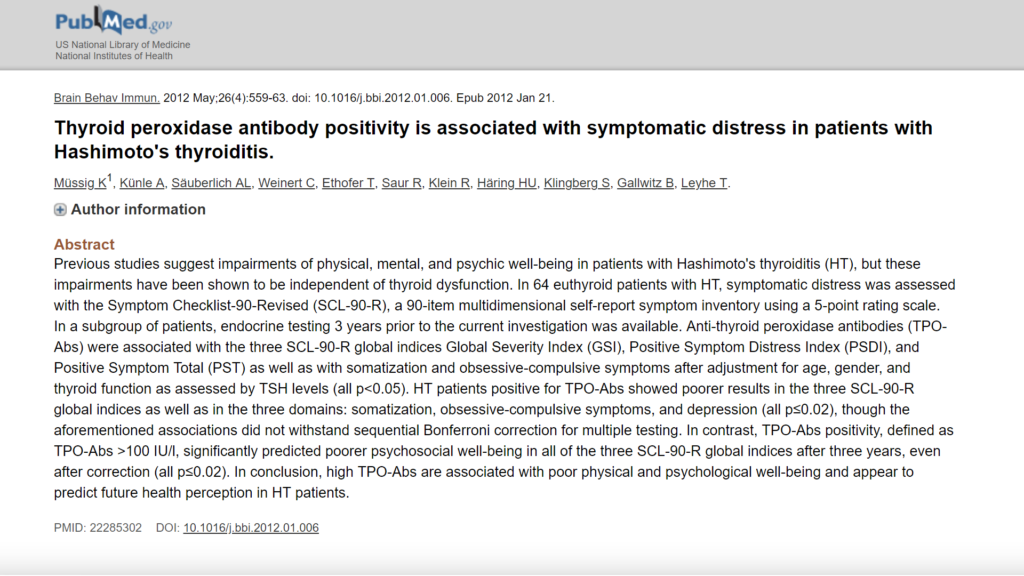
Now, in contention to this, some may cite a paper from the Journal of Brain Behavior and Immunity in 2012 (2) wherein the authors concluded, “TPO positive antibodies, defined as TPO antibodies above 100, significantly predicted poor psychological well-being.”
Now, if we dig into the details… This first would suggest that a TPO antibody should not be above 100, but the devil is in the details here. The authors defined positive as over 100. So they were actually saying that those with positive TPO antibodies had poor psychological well-being. This can be misconstrued because when you look into the details the average level of TPO, for those who were TPO positive, was 1122.
So while they concluded that being positive, aka having TPO antibodies above 100, was associated with poor psychological well-being, the actual average level of antibodies in this group of patients was 1122. So that’s an important detail. So this further supports that TPO antibodies below 500 could be considered a clinical win.
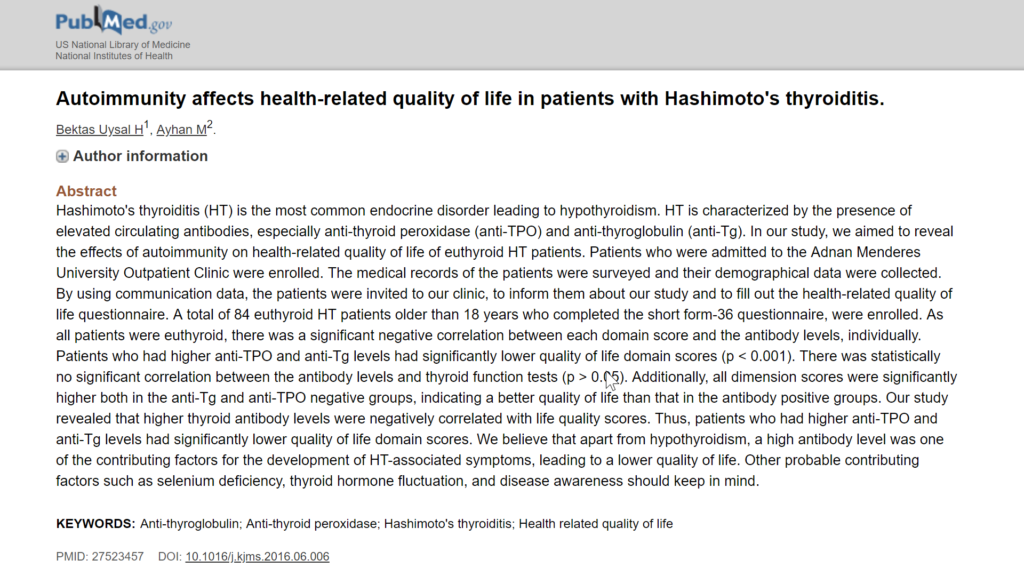
Now, another study did find a TPO of 290, (3) so about 300, was associated with a poor psychological well-being. And the thyroglobulin or TG antibodies of 25—remember normal is 1.0 is below—was also associated with poor psychological well-being. And this held true, independent of thyroid hormone levels. So that’s important to understand that this impact on psychological well-being does not appear to be due exclusively to thyroid hormone levels but may also operate independent of thyroid hormone levels.
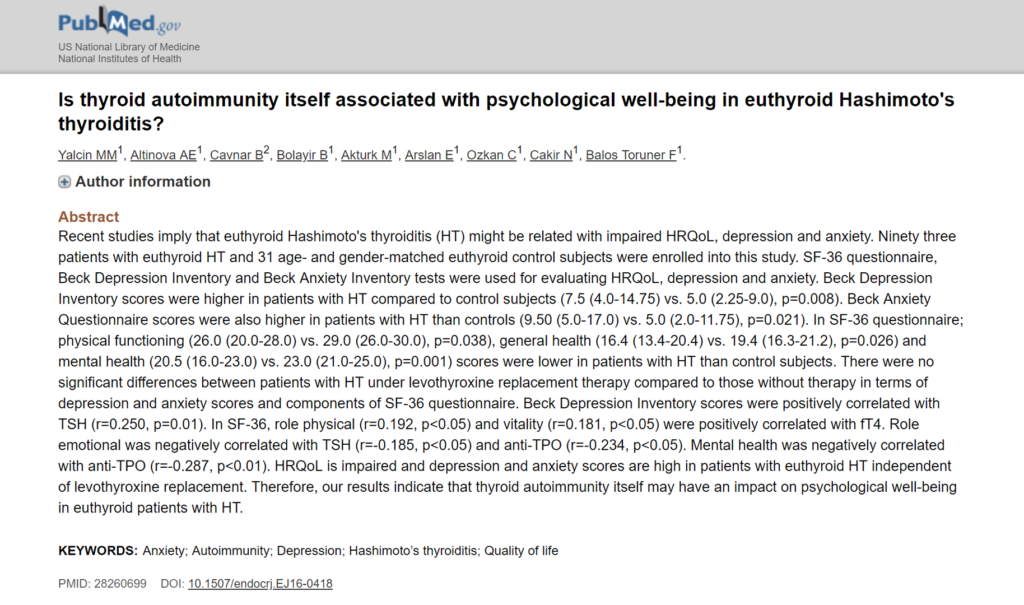
So that is important to understand and also other studies have found something similar. (4) So what this suggests is being the most liberal with our analysis here, we could say that perhaps about 300 would be the level at which we would want to aim for. So 300-500 may be considered a clinical win. So there is some evidence showing a slightly lower elevation of TPO than 500, in this case about 300, is associated with poor psychological well-being. That’s quite different than saying someone is in the low 100s, 100, 200. And you may start getting into the gray area when you get to around 300. Ok.
So coming back to our conclusion. Roughly between 100 and 300 is considered a clinical win. The normal reference range is below 35. The higher the levels the greater the risk in developing true hypothyroidism in the future and the risk of impaired sense of well-being. Thyroglobulin, less than 10 times the reference range is a likely clinical win. The normal reference range, again, is below 1.0. There’s much less data here, so don’t look at these as strongly.
So again, the conclusion. There’s a relationship between thyroid antibodies and the risk of hypothyroidism and depressed well-being. However, this appears to only apply when there is a significant positive; low-level positive may not pose risk. So don’t freak out about mildly-elevated antibodies, especially if you are already eating well and feeling healthy. Key, key point. Do not freak out if you’re generally feeling well and you have TPO antibodies in the low 100s.
Now, what do you do if you’re at 400 or 500 or in the high 100s or low 1000s? Then you want to act. And we’ll come back to some actionable items there in a moment. I’m not trying to paint a picture that you should never act on your thyroid antibodies; I’m trying to help establish when we should be motivated to take action and when we should be happy with where we are. Thus, alleviating that psychological burden and allowing one to enjoy their life and stop working on their antibodies, in air quotes here. Ok.
Sponsored Resources
DrMR: Hey, everyone. I just wanted to say thank you to Biocidin, who has helped make this podcast possible. If you’re not familiar with Biocidin, they have a quality line of products, including anti-microbials, a soil-based probiotic, and a gut detox formula, amongst other things.
And how I came to learn about Biocidin was actually after a few patients of mine—who had been reacting to all other forms of anti-microbials—went out, did some experimentation, and actually found the only anti-microbial formula that they did not negatively react to was Biocidin. So this got me to open my eyes and give them a further look.

And they have a few products I think are worth mentioning. One is their anti-microbial Biocidin, which comes in a few different forms. They also have Proflora®4R, which is one of the few soil-based probiotics that I recommend. And also they have Dentalcidin, which is their Biocidin in the toothpaste form. And this may actually help with the removal of oral biofilms.
Now, if you go to Biocidin.com and you use the code RUSCIO, they will give you free shipping and a free bottle of Dentalcidin when you purchase their comprehensive cleansing program. They do have wholesale pricing available for licensed healthcare practitioners if you email [email protected]
So Biocidin definitely has some helpful products for improving your gut health. And I would definitely recommend checking out Biocidin for more information on a few of these tools that can help you in optimizing your gut health.
Hypothyroid vs Hashimoto’s
Hypothyroid versus Hashimoto’s. Hashimoto’s means you have elevated antibodies, most commonly TPO and thyroglobulin and/or ultrasound changes to the thyroid gland, specifically hypo-echogenicity, meaning there is a lack or there is less echo when ultrasound examination is performed because there is some damage and scarring in the gland. So the gland becomes denser and harder so there’s less of an echo. If you have healthy thyroid follicles, these are kind of like these hollow grapes of thyroid tissue. When they become infiltrated by inflammation and immune cells and subsequently form some scar tissue, they become denser, harder, and there’s less of an echo because of the increased density.
Hashimoto’s is a process wherein your immune system or immune cells damage your thyroid gland. You can have Hashimoto’s and have normal thyroid function. You can have Hashimoto’s and be perfectly healthy; however, as we discussed, there is an association to depressed well-being and highly elevated antibodies above 500, moderately increased risk of developing hypothyroidism in the future.
Hypothyroidism means you have a high TSH paired with low free T4, according to the conventional ranges. Most cases of hypothyroidism require medication to restore normal blood levels of thyroid hormone. And hypothyroidism correlates with a number of symptoms. Let’s go into some of these because this is another area where I think people are confused. And unfortunately, every symptom under the sun, it seems, is leveraged as a way to convince someone they have a problem with their thyroid and sell thyroid books or thyroid supplements or what have you.
Hypothyroidism Symptoms
Now, the increased awareness of thyroid disease is important, and that can help people obtain solutions to help them feel better. However, I fear we’ve gone too far in this direction and now people are blaming everything from their eyebrows to their lack of sex drive to hypothyroid. And you come to a point where any symptom can be attributable to hypothyroidism. And people are just self-diagnosing based on a symptom and there’s not really any support for that kind of arbitrary symptom to diagnose hypothyroidism.
However, there is an evidence-based questionnaire, thankfully, in existence. So to quote, “We identified 13 hypothyroidism-associated symptoms. Globulus sensation”—the feeling of something being stuck in the throat—“difficulty swallowing, anterior neck pain, wheezing, shortness of breath and palpitations”—or like a racing heart feeling—“constipation, hair loss, dry skin, and restlessness. Mood lability”—meaning your moods go up and down—“tiredness and vertigo.”
Now, here’s a key point. Reporting three or more of these symptoms was significantly associated with autoimmune hypothyroid. And also, even more key here, if fatigue is not present, then hypothyroidism is unlikely and if dry skin is not present then hypothyroidism is not likely. So you have to have—the likelihood of hypothyroidism is significant if one has fatigue and/or dry skin combined with a total of three of these symptoms.
So you need to have three of all of these symptoms present and one of those must be either fatigue or dry skin to really support hypothyroidism via a symptomatic diagnosis. So hopefully, this will be a little bit helpful in identifying symptoms that can be useful. If you combine that with an easy assessment that we just discussed, it’s fairly easy to diagnose hypothyroidism. It’s not that challenging.
And unfortunately, again, people oftentimes are led to believe that all their symptoms are being caused by hypothyroidism. And unfortunately, some have discarded practical methods of analysis, and this leads people on a witch hunt for hypothyroidism which can be unfruitful. Because if the problem is not hypothyroidism but you’re trying to force it to be the cause of your problem, if you end up treating what is not the cause of your problem, then the probability of you improving is extremely low. Ok.
True Hypothyroid vs Functionally Low Thyroid
Now, here is a key point. I said a moment ago that it’s fairly easy to define and test for and identify true hypothyroidism. But there’s also this “functionally low” hypothyroidism. And this is where we run into a lot of problems. So, again, true hypothyroidism means you have high TSH paired with low free T4 according to the conventional ranges. Functionally low hypothyroidism means your results are normal according to the conventional ranges but might be toward the higher or lower end of the normal range.

Continuing, you need to know which you are. If you work with a progressive-minded provider and they start you on thyroid hormone, make sure you ask them are you suggesting medication because I am true hypothyroid or as a support because I am functionally low hypothyroid? This matters because one is a disease, and the other is not. One indicates gland damage and the other could merely indicate you are stressed, inflamed, not eating enough or have an issue in your digestive tract.
Now, the latter of these two doesn’t require thyroid medication. However, it may be helpful for a short term to help you feel better, but medication is not required. And these issues can be fixed, meaning a gut issue, not eating enough, inflammation, stress. And then you won’t need medication any longer or you never really needed the medication to begin with and it’s important to understand that because—well, I’ll go into that in a moment here.
I have seen a number of patients who were given the thyroid prescription—Synthroid, Nature-Throid, levothyroxine, WP Thyroid—because they thought they had hypothyroidism and, thus, thought they needed it for life. When, in fact, they never had true hypothyroidism, and they were actually using the prescription as a support. And thus, they would’ve been able to come off of it with no problem, but the provider never disclosed that to them.
So what happens sometimes is someone does not have—and this happens more than I’d like to admit in terms of what I’ve seen in the clinic in picking out these cases. Someone does not have true hypothyroidism. They have functionally low hypothyroidism. So they are given thyroid hormone as a support. They don’t actually need it. It’s like giving testosterone to someone who’s looking to get a little kick in their sex drive or strength. They don’t need it. They don’t have a diagnosed condition of hypogonadism where they need testosterone, but it could be used as a support for a boost.
But the patient wasn’t made aware of this. Or unfortunately, maybe some clinicians don’t fully understand this. And the patient is walking around, thinking that they have to be on thyroid medication forever. And they come into my office five, 10 years later, and we identify that they’re not true hypothyroid, they haven’t needed this medication, they can come off the medication. And that’s a huge realization to achieve because now you don’t think that you have a disease. You don’t think you have thyroid disease, and you can come off of the medication, which by the way is not without risk.
There’s some evidence showing a slight risk with thyroid hormone medication. I think overall these medications are very safe. But we don’t want you to be on something unless you have a need for it. So hopefully, that makes sense. This is an important issue. It’s important not to be walking around, thinking that you have hypothyroidism when you don’t. And again, how you can figure this out, if you want to know how to figure this out for yourself is you can look at your labs from before you started on the medication.
What To Do
Once you’re on the medication, you can’t get a read for what your gland was doing because it’s skewed by the hormone that you’re taking. Look at your labs from the time of diagnosis, from before you started on the thyroid medication. And if you do not have conventional range high TSH paired with conventional range low free T4, then you do not have true hypothyroidism, and you likely have functional hypothyroidism. And there is a very high probability that you do not need and will not need your thyroid medication.
Now, I want to be careful in saying you need to run this by your doctor. I wouldn’t go out and just try to do this on your own. Run it by a healthcare provider, so they can make or update the diagnosis. But I want to arm you with the knowledge so that you can prompt the investigation with a competent clinician who can then render the diagnosis and the recommendation. Ok.

So what to do? Identify if you are true hypothyroid. If yes, start on medication. A T3/T4 combination may work better for some but not for all. And I’ll be releasing either an article or a podcast on this soon—a review of the literature—on the T4/T3 combination. And for those of you who are not familiar with this, let me take a step back and just explain that. The thyroid gland produces two forms of hormone: T4 and T3. But most of the T3 is actually produced outside of the thyroid gland when your body converts the T4 into T3 in the periphery of the body.
Some people don’t adequately convert T4 to T3, and therefore, may do better on a medication that has a combination of both T4 and T3. However, I fear that the need or T4/T3 medications has been slightly overstated. There are definitely people who will do better on a T4/T3 combination but not for all. So without getting too far into that issue: start on a medication. You can start with either T4 alone like levothyroxine or Synthroid or something that combines both: Nature-Throid, Armour, or you can add something like Cytomel which is T3 alone onto your levothyroxine or Synthroid which is T4 alone.
Sensitive patients or reactive patients may do better on a cleaner form of thyroid hormone that’s devoid of fillers and excipients and binding agents. Nature-Throid may be the best option there.
Now, if you’re not hypothyroid, look to other systems of the body as a cause of your symptoms. And here, this may be a female hormone imbalance. It may be a digestive tract issue. I would say digestive issues are probably the most common. But female hormone imbalances are also fairly common. That may be causing your symptoms. Also, don’t forget the foundational issues of your diet, your sleep, exercise, stress, enjoyment in your life. Those things, of course, can cause some of the symptoms that are sometimes attributed to hypothyroidism.
Next, identify if you have Hashimoto’s. Antibodies over 300-500 for TPO: take action to improve your antibodies. Under 300-500, no action is required or consider action if none has been taken previously. Now, regarding what you can do. A low-carb diet has been shown to be helpful, as has a gluten-reduced diet. I use the term gluten-reduced because I think we need to be more discerning with our language regarding gluten. Sometimes when we say gluten-free, people take that as a mandate to never have any gluten for the rest of your life. And I think that recommendation is a bit overzealous.
Now, I do understand that there’s an association between hypothyroidism and Hashimoto’s and celiac disease. That’s true. But it’s not to say that 100% of people with thyroid problems need to eat as if they have celiac disease. And we may be able to garner the benefit with a simple reduction of gluten, meaning you can have some on occasion. And I know this may sound overly simple, but sometimes the best recommendations are the most simplified.
You should avoid gluten in correspondence with your level of reactivity, meaning the worse your reaction to gluten, the more strict you should be in avoiding it. The less reactive you are, the less strictly you have to avoid it. We have discussed previously a multi-center Italian study that looked at over 12,000 patients and found that over 90% of people who experienced a reaction to gluten, experienced that reaction to gluten within 24 hours.
Why is that relevant? It’s relevant because sometimes the remark is made that if you have any autoimmunity you can never have gluten because you may have no symptoms but you may be fueling the autoimmune process and you may not notice any symptomatic change for months or years. Ok. That’s one argument. I don’t see great evidence to support that. In fact, in this study which is probably the best one we have of its kind where a group of doctors tried very hard to identify the symptoms and they tracked these patients, they did multiple visits, they used questionnaires, they used testing.
They found that over 90% of patients who had a reaction to gluten had a discernible symptomatic reaction within 24 hours. So that tells me that for most people you will notice some kind of negative symptoms, and you will notice those within 24 hours. And if you don’t notice anything, you can have some gluten. And I think that’s pretty reasonable. It’s pretty reasonable to conclude that if you’re damaging your body with a food, you’ll notice some kind of symptomatic reaction. It might be skin. It might be clarity. It might be energy. It might be joint pain. And this is what the research also shows, but there will be a discernible, symptomatic reaction within 24 hours for the vast majority of cases, at least based upon the best evidence that we have.
Now, if you have Hashimoto’s, some supplementation can be helpful. And all of these have been shown in at least one clinical trial to be helpful in lowering the antibodies associated with Hashimoto’s, TPO and TG. Vitamin D, selenium, magnesium, and CoQ10. And also, looking at your gut health. We have one study, albeit the data here is mixed, showing eradication of H. pylori or treatment of H. pylori can help to significantly lower antibodies and also some findings that there’s a fairly high association between hypothyroidism and small intestinal bacterial overgrowth. And one case study, I’m sorry, that looked at the treatment of Blastocystis hominins, and this yielded an improvement in both symptoms and thyroid autoimmunity.
Selenium
Now regarding selenium. If selenium deficiency was a cause of decreased quality of life, then we should see improvements in quality of life with selenium supplementation. (6) Now, while not all the data here agree, there is data to support a three- to six-month use of selenium for both quality of life and thyroid antibodies. The reason why this is relevant is because we have a lot of information showing that we can decrease thyroid antibodies—I shouldn’t say a lot, but we have a handful of clinical trials showing that we have natural medicines to decrease thyroid antibodies.
It’s also important to tie that change on a lab to someone feeling better. So this is where it’s nice to see that selenium, in addition to lowering thyroid antibodies, does have some documentation showing an improvement in quality of life when used for three to six months in duration.
Dr. Ruscio Resources
DrMR: Hey, everyone, this is Dr. Ruscio. I quickly wanted to fill you in on the three main resources that are available to you in case you need help or would like to learn more. Of course, I see patients both via telemedicine, via Skype, and also at my physical practice in Walnut Creek, California.
There is of course my book, Healthy Gut Healthy You, which gives you what I think is one of the best self-help protocols for optimizing you gut health and of course understanding why your gut is so important and so massively impactful on your overall health.
And then finally, if you are a clinician trying to learn more about my functional medicine approach, there is The Future of Functional Medicine Review, which is a monthly newsletter. Which is a training tool to help sharpen clinical skills. All of the information for all three of these is available at the URL drruscio.com/resources. And in case you are on the go, that link is available in the description on all of your podcast players. Okay, back to the show.
Case Study Hypothyroid Hashimoto’s
So kind of rounding out some of the edges here. What to do? If you are on thyroid medication and your TSH and free T4 are within the conventionally normal ranges but you are still not feeling well, look to your gut health. Or if you have TPO antibodies in the low 100s but are still symptomatic, look to your gut health. Optimizing your gut health can lead to a reduction of thyroid medication. I’ve seen this a number of times—and you see some of this being reported in the medical literature—that different gastrointestinal conditions can cause malabsorption of the medication. And by rectifying those, you can have an improvement in your absorption of the medication, therefore a decrease in the dose.
Optimizing gut health can also lead to improvements in autoimmunity and can lead to improvements of nonresponsive hypothyroid. I’m putting those in quotes here. Hypothyroid-like, I should say, symptoms. Remember that perception of health impacts health outcome or health outcomes.
So thinking you are unhealthy will impact your health in a measurable way. This is why it’s important to understand if you have TPO antibodies in the low 100s, it doesn’t mean that you’re sick or you have a disease. It’s also important to understand that if you have functionally low hypothyroidism, you don’t necessarily have a disease or an overt medical issue.
This is important because we all have the tendency to internalize the diagnoses that we’ve been given. That anguish can have a negative impact on your health. So it’s important to be progressive, yes, but also make sure that we are being grounded and practical and discerning in the language that we use and the diagnoses that we make.

So briefly here, just to talk about June. (7) When June came in, she had hypothyroid and Hashimoto’s. And we also found H. pylori, Epstein-Barr, which both may contribute to Hashimoto’s. However, after treatment, there was actually no change in her thyroid antibodies, and there was no change in her H. pylori markers. However, she had lost weight, improved sleep, and had better digestive function.
So this is important to understand that you can become much healthier even if your lab results don’t change which is why I don’t recommend harping on lab results.
Case Study Thyroid Nodule

Now, Patricia’s story. (8) She had gone to her primary care physician for a thyroid nodule which was causing some swelling. She felt like she couldn’t breathe at night. The doctor said she could have an operation but that it may or may not alleviate her symptoms. And she would probably have to go on medication after the surgery.
In her case, simple dietary changes, namely the paleo diet, completely resolved her issue in a number of weeks. Now, her issue may have been due to swelling in the thyroid from the foods that she was eating. She may have also had a condition known as eosinophilic esophagitis which could present as symptoms similar to this.
But in any case, she had marked improvements with just simple dietary changes, and we did not have to do a crazy lab evaluation to try to discern this elaborate esoteric web of cause. Sometimes you have to, yes, but don’t forget about the power of the simple fundamentals. And in her case, she did very well with just some simple dietary changes.
Case Study Hashimoto’s

And then we have Laura. (9) And Laura was suffering from energy ups and downs, waking, insomnia, joint pain from arthritis, and we also found that Laura had Hashimoto’s. We shifted Laura away from her previous vegetarian-like diet towards more of a paleo-like diet. We also used some herbs and vitamins to help quell inflammation in the thyroid, like we discussed a moment ago, in addition to herbal support for her female hormones, also like we discussed a moment ago.
Now, in two months, Laura lost a significant amount of weight, was sleeping much better, and had improved well-being and much less joint pain. After improving her gut health, Laura required less thyroid medication. She was able to cut her dose of thyroid medication in half and felt better than when she was on a higher dose of thyroid medication. That’s a key point. Sometimes there’s this mistaken thinking that you need to be on more thyroid hormone or have your thyroid hormone levels at the upper end of the normal range. And that’s not always true.
In Laura’s case, she felt much better by every measurable parameter, both symptomatic or objective, and she was on half the dose of thyroid medication. This illustrates how improving your gut health can improve a litany of symptoms and decrease the amount of thyroid medication that’s needed. So we can use natural medicine to improve your health, but we also want to be careful to avoid the overzealousness and fear-mongering that unfortunately permeates some circles of thyroid care.
Now to optimize your gut health, I have my book Healthy Gut, Healthy You. If you’re a clinician and you want to learn more about this approach, you can see my monthly clinical newsletter, the Future of Functional Medicine Review. And you can also check out our website at DrRuscio.com for weekly podcasts, articles, and videos.
Episode Wrap-Up
And I just want to leave you this in close. Pursue your purpose. “He who has a why to live can bear almost any how” by Friedrich Nietzsche. I think that’s an amazing quote, and it’s important to remember that we’re trying to use our health to get back to our life. And it’s important to have a life to get back to, something bigger than you that you’re trying to do, that you enjoy and that you love.
Sometimes it’s easy to get pulled into a black hole of health research, but don’t forget about the bigger purpose, what you’re trying to do in your life. And if you haven’t found that yet, I would put some time and energy into that because that can yield huge dividends. And it’s important to have something to put this energy that you’ll cultivate with improving your health into.
This is Dr. Ruscio, and I hope this helps you navigate this tumultuous landscape of thyroid and provide you some clarity along your journey. And if you need anything, feel free to comment or reach out to our office. Probably the most helpful thing I can offer you is go through the protocol in Healthy Gut, Healthy You. That can do volumes to help improve your health, both gut and thyroid, because remember the gut is very impactful on the thyroid. And that is it, guys. I will talk to you next time. All right. Thanks.
Dr. Michael Ruscio is a DC, natural health provider, researcher, and clinician. He serves as an Adjunct Professor at the University of Bridgeport and has published numerous papers in scientific journals as well as the book Healthy Gut, Healthy You. He also founded the Ruscio Institute of Functional Health, where he helps patients with a wide range of GI conditions and serves as the Head of Research.➕ Resources & Links
- Anti-thyroperoxidase antibody levels >500 IU/ml indicate a moderately increased risk for developing hypothyroidism in autoimmune thyroiditis
- Thyroid peroxidase antibody positivity is associated with symptomatic distress in patients with Hashimoto’s thyroiditis
- Autoimmunity affects health-related quality of life in patients with Hashimoto’s thyroiditis.
- Is thyroid autoimmunity itself associated with psychological well-being in euthyroid Hashimoto’s thyroiditis?
- Hypothyroid symptoms and the likelihood of overt thyroid failure: a population-based case-control study
- Insufficient documentation for clinical efficacy of selenium supplementation in chronic autoimmune thyroiditis, based on a systematic review and meta-analysis
- Thyroid autoimmunity and H. pylori – One Patient’s Story
- Thyroid nodule success
- Take less thyroid medication and feel better by improving gut health – Laura’s Story
Discussion
I care about answering your questions and sharing my knowledge with you. Leave a comment or connect with me on social media asking any health question you may have and I just might incorporate it into our next listener questions podcast episode just for you!