The Most Accurate Thyroid Tests & How Healing Your Gut Can Fix Your Thyroid: A Case Study
Written by ![]() Dr. Michael Ruscio, DC on
September 12, 2018
Dr. Michael Ruscio, DC on
September 12, 2018
If you are using the wrong thyroid test you could miss the fact that you are hypothyroid because your labs say you are normal. The best test to use is known as the dialysis/LC-MS (I will explain what that means momentarily). It’s also important to understand when your thyroid-like symptoms are being caused by your gut, not your thyroid. I will share a case study where 100% of thyroid-like symptoms cleared after improving the patient’s gut health.
Episode Intro
Dr. Michael Ruscio, DC: Hey, everyone. Welcome to Dr. Ruscio Radio, and this is Dr. Ruscio. And today let’s dig into what’ll hopefully be some insightful information regarding gut and thyroid.
First, I’d like to discuss with you a review of a research paper, which has outlined the fallibility or/nor the act of accuracy with some of the standard methods for testing T4 and in T3.
And also, I want to illustrate a case study, which helps answer the question, do we treat the gut first or do we treat thyroid first? And this was a great case, since not always one or the other. Oftentimes, treating the gut first makes the most sense, but not always. But this case was a prime example of how you can see abnormalities in a thyroid test that are actually just a manifestation of a problem in the gut.
[Continue reading below]
Dr. R’s Fast Facts Summary
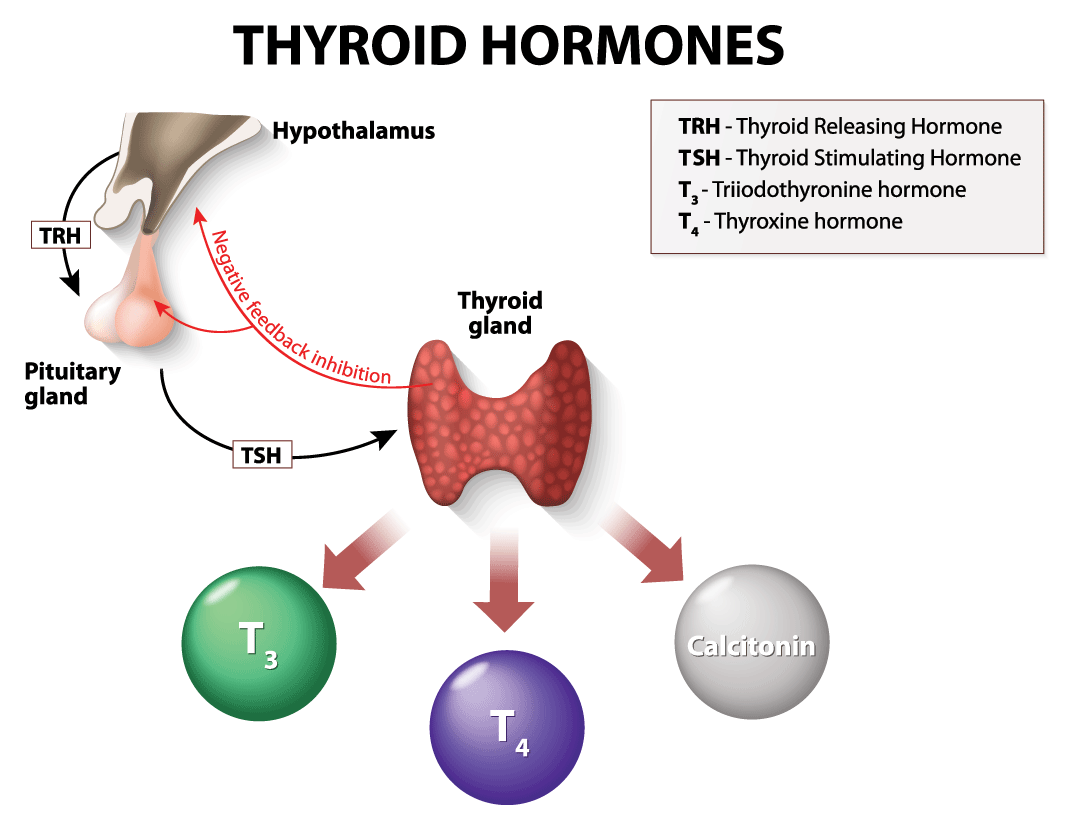
Testing for Thyroid
- Standard immunoassay technology – the default test for Thyroid
- Some might have an imbalance that is only able to be identified when using a different form of testing known as Dialysis with Liquid Chromatography Mass Spectrometry.
- Filters out binding proteins in the blood that can skew results due to stress, inflammation, and medication use
- The binding proteins can make someone who is Hypothyroid look like they have normal thyroid
- Until you filter out the blood using this methodology you may not get an accurate read on the patient’s true state
- Study: DIAGNOSIS OF ENDOCRINE DISEASE: How reliable are free thyroid and total T3 hormone assays?
- The dialysis method may also help to identify formally subclinical hypothyroid cases as frank hypothyroid thus assisting in the decision to initiate thyroid hormone medication
- Lower T3 values when tested with Dialysis method compared to immunoassay method in patients with TSH over 4.5
- TSH and symptoms may more closely track with dialysis T4 rather than the immunoassay T4
- The dialysis method may also help to identify formally subclinical hypothyroid cases as frank hypothyroid thus assisting in the decision to initiate thyroid hormone medication
Case Study
Patient – 32 yr old Female
- Previous diagnosis – Hashimoto’s and PCOS
- Previously treated for SIBO and Blasto
- Symptoms – bloating, constipation, weight gain, mental fog, abnormal cycle length, PMS, Premenstrual pain
- Positive for Candida via IGM antibodies
- Low positive TPO antibodies
Testing
- Standard GI work up for dysbiosis and GI pathogens
- Standard blood and urine analysis CBC with differential
- Comprehensive metabolic panel
- TSH, free T4, Vit D, Thyroid antibodies and Thyroid metabolites
Dietary Recommendations
- Start with Paleo/Low FODMAP diet (1.5 weeks prior to starting supps)
- Try to wean off coffee
Supplementation Program
- Omega 3.6.9 blend and Vitamin D with K
- Herbal blend for estrogen and progesterone
- Lacto Bifido blend probiotic & S. boulardii
- Digestive enzyme w/ HCL and Betaine HCL
Sequencing Treatment
- Begin diet only for 1.5 weeks
- Start supplements 1.5 week before follow up
- This initial program will help replete deficiencies, start balancing female hormones and start the process of addressing any intestinal dysbiosis
Test Results
- SIBO, Yeast and Blasto
- Autoimmune thyroid – TPO antibodies 45 (acceptable level) but T4 (free and total) were low
Patient Response
- Responded very well to diet
- Minimal response to program
Starting Antimicrobial Protocol
- Herbal antimicrobials, Artemisinin (anti- blasto agent), Anti-biofilm agent, Magnesium citrate
- Increase probiotics
- OB started her on progesterone
5 Week Follow Up
- Improved: Bloating, Distension, Body weight, Mental fog, Constipation, Skin, PCOS
- Cycling improved
- No symptoms were non-responsive or worse
Maintain Plan and Follow Up in 2 Months
- Dietary reintroduction
- Come off herbal estrogen and progesterone
- Find minimal items needed in your program
- Get help with fixing your thyroid.
- Get your personalized plan for optimizing your gut health with my new book.
- Healthcare providers looking to sharpen their clinical skills, check out the Future of Functional Medicine Review Clinical Newsletter.

Subscribe:
Download Episode (Right click on link and ‘Save As’)
And so this case, presented with GI findings plus thyroid hormone imbalances, the remedy was focusing on the gut and actually some female hormone support to right those imbalances. And this is the key point because I often see people treating the thyroid when the thyroid is a symptom of a cause somewhere else in the body rather that being the cause of the actual problem. And hence, people treat the thyroid and symptoms don’t improve.
Future of Functional Medicine Review
So we’ll jump into some of these details here in a minute. I want to point out that both of these two areas of information are taken directly from the Future of Functional Medicine Review clinical newsletter. And if you’re not aware of the Future of Functional Medicine Review, this is a monthly publication that I put out in my attempt to help give you very clinical information. We summarize one case study and a number of research studies that are all very impactful for being a better functional medicine provider.
 And again, what we will cover are direct derivatives of back issues or previous issues of the Future of Functional Medicine Review. And during the month of September, if you want to sign up, you can sign up for $1. And that would give you your first month of access. And you can read through the current issue. And you can you can read through all of the previous issues, nearly two years of content. There is a ton of information contained in this guys.
And again, what we will cover are direct derivatives of back issues or previous issues of the Future of Functional Medicine Review. And during the month of September, if you want to sign up, you can sign up for $1. And that would give you your first month of access. And you can read through the current issue. And you can you can read through all of the previous issues, nearly two years of content. There is a ton of information contained in this guys.
And I’m very happy to say that there are now clinicians who have been applying this methodology and able to obtain excellent result for patients or clinicians that they work with, with a really minimal amount of effort and expense. In fact, Robert Abbott recently provided one of his case studies. Robert Abbott is a medical doctor and medical resident, wherein he was able to help someone with gut and female hormone related symptoms with a very simple minimal testing protocol and was actually able to get her quite remarkable results.
So, the lessons embedded in the newsletter are able to be applied to the practices of others, which, thankfully, because that’s really the goal.
So, in any case, if you want to be able to access all these, you can go over to drruscio.com/review. We will also put that link in all your podcasts player descriptions in case you’re on the go. And you can sign up for $1.
Thyroid Study
But let’s continue now into the body of this podcast here. So, to the question of, how reliable are T4 and T3 testing? This comes from the February 2018 issue of the Future of Functional Medicine Review. And there’s a couple of really important things here to consider. Now, you’ve heard me say and criticize the over testing ethos that exists in functional medicine. However, testing can be helpful. It’s just we need to use the right testing at the right time. And when we do that, that’s when testing can really help us be more effective in the interventions that we undergo.
And a key area here is thyroid. And the real take home is that the standard assessments that are utilizing what’s known as an immunoassay technology. So if you go to LabCorp or to Quest or if you some intermediary like Direct Labs, that I believe goes to ultimately uses LabCorp. Then the default test is often the methodology wherein they use the immunoassay. And this isn’t necessarily a bad test. But for some people, they may have the imbalance that is only able to be identified when using a different form of testing.
Chromatography Mass Spectrometry
And this form of testing is known as dialysis with liquid chromatography-mass spectrometry. It’s a mouthful. But essentially, what this form of testing will do is it will filter out binding proteins in the blood that can skew due to stress or inflammation or medication use or various disease states. And these binding proteins can actually make someone who is hypothyroid look normothyroid. So until you filter out these confounding particles in the blood with this dialysis methodology, you may not be able to get an actual or accurate read of what one’s blood thyroid hormone levels look like.
And so, I’ll share with you a quote from—well, essentially, the way I write the research review section of the Future of Functional Medicine Review, to make it as easy for you as I can, is I list a statement for you in plain language. And then after that statement, I give you a couple of bullet points that are direct quotes from the research papers that reinforce that statement.
So here’s the simple statement:
“The dialysis method may also help identify formally sub-clinical hypothyroid cases as frank hypothyroid, thus assisting in the decision to initiate thyroid hormone medication.”
Okay, so that’s kind of a simple sentence.
 Now, here’s a couple of the quotes right from the paper that illustrate that:
Now, here’s a couple of the quotes right from the paper that illustrate that:
“Jonklaas et al. reported lower T3 values when tested by the dialysis method compared to the immunoassay method in patients with TSH over 4.5.”
Translation: in patients with mildly elevated TSH, their T3 looked normal when they were tested on a regular blood test. But when using the dialysis method, they actually came back low, hence, labeling them as true hypothyroid.
Another quote:
“Patients with high concentrations for TSH often had thyroid hormone levels below the reference interval when tested via the dialysis method but were classified as normal when tested by the immunoassay.”
So, again, we’re seeing that there are some cases where they may only identify as hypothyroid when tested by this more sensitive methodology.
And one more quote here: A study of 40 patients classified as sub-clinical hypothyroidism—now remember, sub-clinical hypothyroidism is when your TSH is high and your T4 and T3 are normal or your T4 is normal.
“A study of 40 patients classified as sub-clinical hypothyroid by elevated TSH with normal free T4 levels by conventional immunoassay found that 65% of such patients actually had free T3 or free T4 levels below the reference range when tested by the dialysis method.”
And I link for you to this specific paper that they’re citing here in the notes. So, this is really important stuff. And I think it’s very helpful to look at this actual outcome data showing that, yes, there are real cases who will be misclassified when not using this more sensitive methodology of thyroid assessment.
Sponsored Resources
 Hey, guys. We’ve discussed at length the benefits of probiotics. But it can be hard to know which specific probiotic products to use. One probiotic that I endorse is Just Thrive Probiotic. Just Thrive is one of the few category three (aka soil-based) probiotics I recommend. In fact, one exciting study has found that the strains in Just Thrive Probiotic can begin healing leaky gut.
Hey, guys. We’ve discussed at length the benefits of probiotics. But it can be hard to know which specific probiotic products to use. One probiotic that I endorse is Just Thrive Probiotic. Just Thrive is one of the few category three (aka soil-based) probiotics I recommend. In fact, one exciting study has found that the strains in Just Thrive Probiotic can begin healing leaky gut.
They also have some very exciting research coming in the future. If you haven’t listened to our podcast with Kiran Krishnan who is performing some of this research, you should definitely check it out.
And good news! If you’d like to try Just Thrive, they’re offering 25% off your first purchase when you use the code RUSCIO at checkout (R-U-S-C-I-O). They’re available at ThriveProbiotic.com or on Amazon. Check them out.
And then here’s on bullet point, kind of the plain language bullet point, and then I’ll follow with a quick quote: TSH and symptoms may more closely track with dialysis T4 rather than the immunoassay T4. Okay, so we’ve already kind of hinted at that. And here’s the quote that reinforces that:
“These papers have shown a poor correlation of immunoassay values for free T4, free T3 and total T3 with TSH as well as with the patients clinical condition.”
So, essentially, what they’re saying is, the standard testing has a poor correlation to TSH. However, the dialysis method has a better correlation to TSH and, most importantly, to patient’s symptoms. Because you know that I harp on the outcome data. So the outcome data here that’s most important is how this correlates with how someone is feeling.
So, for clinicians, I think this type of information is very helpful because you can see the direct evidence supporting the approach that I’m recommending. Also, in some of the earlier issues of the Future of Functional Medicine Review, I provided the exact links to order this tests through LabCorp and Quest. So, if you’re a layperson, you’ve likely heard this and you may want to inquire about it. If you’re a clinician, you would likely like to see some of the evidence behind that and be able to actually access the lab tests to effectuate these markers. And so, this is provided, of course, in the write up in the Future of Functional Medicine Review.
Case Study
Now, let’s move on to a case study. And this case study, as I mentioned a moment ago, helps answer the question of when we’re seeing gut imbalances and thyroid imbalances, what do we do? So, the patient, her name was Kaitlyn. She’s a 32-year-old female. Her previous diagnosis included Hashimoto’s. She was on no medication. And her chief complaints were bloating at an eight out of 10 severity, abdominal distention at an eight out of 10, weight gain at a five out of 10, mental fog at a seven out of 10.
And then, also some symptoms that she didn’t report but—I look at people’s chief complaint and then I have another column where I track other symptoms I’ve picked out of their paperwork or out of their exam that I think are important that they may not have mentioned. In this case, she had abnormal cycle length, flow, pre-menstrual pain, and also PMS. So these are important because she’s not complaining necessarily about female hormones. But if you’re reading everything closely—and when I say “reading,” I use that term figuratively—then we could see that there’s definitely some symptomatology that is suggestive of female hormone imbalance.
 So, initial impression: Kaitlyn presents as a 32-year-old female who was generally in good health with a healthy lifestyle and a good outlook on her health. A little overdone there but she could improve her diet however. A few years ago, some of her chief complaints started after a bout of vomiting that had no known cause. And then she gradually experienced development of her chief complaints over time. She had been diagnosed and treated for SIBO and Blasto with only minimal change: one round of rifaximin with neomycin, one round of Flagyl with Bactrim. She also was positive for Candida via IgM antibodies previously. She does also have low positive TPO antibodies, I believe. Well, previously, they come back low positive. So I don’t have the exact value in front of me here but I’m assuming it’s around 100. But she was euthyroid, meaning her thyroid hormone levels were all normal, TSH and T4. And her prior endoscopy was normal.
So, initial impression: Kaitlyn presents as a 32-year-old female who was generally in good health with a healthy lifestyle and a good outlook on her health. A little overdone there but she could improve her diet however. A few years ago, some of her chief complaints started after a bout of vomiting that had no known cause. And then she gradually experienced development of her chief complaints over time. She had been diagnosed and treated for SIBO and Blasto with only minimal change: one round of rifaximin with neomycin, one round of Flagyl with Bactrim. She also was positive for Candida via IgM antibodies previously. She does also have low positive TPO antibodies, I believe. Well, previously, they come back low positive. So I don’t have the exact value in front of me here but I’m assuming it’s around 100. But she was euthyroid, meaning her thyroid hormone levels were all normal, TSH and T4. And her prior endoscopy was normal.
She will likely need standard SIBO care and will respond well since she hasn’t done much outside of antibiotics and has not tried diets or herbal antimicrobials. She has responded slightly to enzymes B12 and iron. Kaitlyn also exhibits symptoms consistent with female hormone imbalances, which seemed to provocate her digestion. So support here should yield good result also. There’s a potential for SIFO, small intestinal fungal overgrowth, due to the Candida antibodies. And there’s also possibility of anti-parietal cell autoimmunity due to the stomach symptoms she’s experiencing and the fact that she has Hashimoto’s, because they tend to go together. There’s a slightly increased probability of maybe 30% that someone will have anti-parietal cell antibodies if they are Hashimoto’s positive. And she has no prior functional medicine care so her prognosis is good to excellent.
Okay. And then list out for you here previous diets – none, previous treatments – rifaximin/neomycin helped; B12 and iron helped slightly; Flagyl and Bactrim, no change; probiotics, no change; enzymes helped slightly. Okay, so her second visit is after I’ve taken some time to look over everything to put together a plan. We laid out the initial testing and treatment recommendations.
Testing and Treatment Recommendations
So we perform an Aerodiagnostics lactulose SIBO breath test, a Diagnostic Solutions GI-MAP test, and then two panels at LabCorp; one, blood, urine, stool, and breath, all looking at a suite of GI markers, and then one blood and urine analysis more of a routine health and wellness panel. And the rationale behind the testing, we will perform our standard GI work up with test for SIBO, dysbiosis, and GI pathogens. We will also order standard blood and urine analysis like a CBC with differential, a comprehensive metabolic panel, TSH, free T4, vitamin D, etcetera. We will also check thyroid antibodies and thyroid metabolites.
Okay. So her recommendations. Dietary: Please start on the paleo low FODMAP diet. Work to wean yourself off coffee and use non-coffee alternatives like tea or natural energy drinks. And some of her symptoms indicate that she may have a problem with coffee, especially when you see bloating and abdominal distention, that may be problematic. And part of what I ask people in their initial paperwork is have they ever taken—if they’re drinking coffee regularly, have you ever taken a break from coffee to see if you feel better off it or do you notice some days when you drink more or less you feel better or worse. Some people will say, ‘’Yeah, if I have more than one cup in a day, I get bloated’’. Well, that may mean you want to throttle back your coffee a little bit.
 Okay. And I’ll see here. So, then supplemental recommendations, we put her on a omega 3-6-9 blend along with the vitamin D with K. we put her on an herbal blend for estrogen and an herbal blend for progesterone. And in the issue of the Future of Functional Medicine Review, we show you the exact product labels that we use. And we also put her on a Lacto/Bifido blend probiotic category one and also an S. boulardii probiotic category two and a digestive enzyme with HCl and also a betaine HCl supplement.
Okay. And I’ll see here. So, then supplemental recommendations, we put her on a omega 3-6-9 blend along with the vitamin D with K. we put her on an herbal blend for estrogen and an herbal blend for progesterone. And in the issue of the Future of Functional Medicine Review, we show you the exact product labels that we use. And we also put her on a Lacto/Bifido blend probiotic category one and also an S. boulardii probiotic category two and a digestive enzyme with HCl and also a betaine HCl supplement.
And I gave her some sequencing notes. Be on the diet for one and a half weeks before starting on the supplement program. There’s also something else I’ve covered in the newsletter, which is ‘sequencing the initiation of your interventions’. And I’ve actually spoken about this at length and you see this evolve in my case studies over the past nearly two years, where now I am sequencing initiation of interventions. Because if someone comes back two days later and they’re feeling noticeable better, I want to know, was it from the diet, was it from the probiotic, was it form both? Did you notice that you felt no change in the diet and then when you went in the probiotics you saw as huge jump?
These things are really important because despite what much of the field of functional medicine would lead you to believe, testing will not tell us who is going to respond on what diet or who is going to respond on what probiotic, but what will a good empirical evaluation, meaning a good read of someone’s response. So this is why it’s crucial to not only listen intently at your follow-up visits but also stagger interventions that you can try to parse out the effect of these different therapies that you may be recommending. So, in this case, we are recommending some treatment and some diet, we stagger the start so I can get a sense.
So, be on a diet for one and a half weeks before starting on the supplement and then be on the supplements for at least a week and a half before following up. And my rationale here is diet is a great place to start, given her GI symptoms. And also, her initial program will help replete deficiencies, start balancing her female hormones, and start the process of addressing any gastrointestinal dysbiosis.
Okay. So visit three, which was probably about four weeks later, her subjective assessment, her symptom assessment. So, in the meantime, she had actually been diagnosed by her OB with PCOS and was instructed to start on, essentially, a prescription progesterone. She noted that the paleo, low FODMAP diet was very helpful for bloating, distention, and mental fog and that the initial program also was very helpful, especially the betaine HCl. Weaning off coffee, she reported no change. And overall improved symptoms included bloating, distention, and mental fog. Symptoms that were the same included constipation, cycle length, flow, PMS, and pain. And none of her symptoms were worse.
Now, looking at her labs. Her labs showed a borderline positive SIBO with a hydrogen elevation of about 26. A mild but what I would consider mostly clinically insignificant elevation of methane of 8 to 9. Although, some evidence will show that correlates with constipation. So that maybe something to move on.
 Now, here’s where it gets interesting, you’ve probably heard me say that we should not look at lab tests overly literally. Because when I run two quality stools assessments or quality GI assessments at the same time, it is rare that they overlap, right. So it tells us that the testing isn’t perfect. And really, what I think the testing can help us do is establish if there is a theme of dysbiosis. And then we can start using some of the treatments in the dysbiosis tool kit. But we should not be looking a stool test results overly literally. I think this is one of the most detrimental practices. And I think time and experience helps guide you out of this. So, it’s not necessarily criticism. But, certainly, I see more people hold themselves back, either clinicians or patients, when they try to intervene, literally, based upon the lab test results. But we should rather be looking, ‘okay, there’s a theme of dysbiosis here now, were going to start poking and prodding and nudging the microbiota with some of the different therapies available for dysbiosis’. And then, using the person’s symptomatic response to tell us which one of those were the best.
Now, here’s where it gets interesting, you’ve probably heard me say that we should not look at lab tests overly literally. Because when I run two quality stools assessments or quality GI assessments at the same time, it is rare that they overlap, right. So it tells us that the testing isn’t perfect. And really, what I think the testing can help us do is establish if there is a theme of dysbiosis. And then we can start using some of the treatments in the dysbiosis tool kit. But we should not be looking a stool test results overly literally. I think this is one of the most detrimental practices. And I think time and experience helps guide you out of this. So, it’s not necessarily criticism. But, certainly, I see more people hold themselves back, either clinicians or patients, when they try to intervene, literally, based upon the lab test results. But we should rather be looking, ‘okay, there’s a theme of dysbiosis here now, were going to start poking and prodding and nudging the microbiota with some of the different therapies available for dysbiosis’. And then, using the person’s symptomatic response to tell us which one of those were the best.
And I know that doesn’t sound—it’s easier to fall into or be sold on the concept of ‘oh, here’s that lab test that told us exactly what to do’. And I can tell you that the practitioners that do that do not get as good of results as the ones who don’t. And in my opinion—and I’m happy to be challenged on that and I’m happy to change my mind if there’s good evidence to support that. But I’ve just seen too many patients who have gone to other doctors and the doctors treated the labs at the partial exclusion of the patient’s symptomatic responses. And they weren’t able to fix the patient. So it’s very important not to look at labs overly literally.
View Dr. Ruscio’s Additional Resources
So, the point I’m driving at here is, the Diagnostic Solutions found Blasto, yet Blasto was not found on the Lab Corp profile. Also, the diagnostic solutions did not find H. pylori, but H. pylori was found via two antibody fractions on the Lab Corp profile. Now, there was overlap for Geotrichum, which is a type of fungus. So that’s good, right? But there’s a bit here that does not overlap, which illustrates my point of not looking at these tests overly literally. And there’s a couple of more findings here, I won’t go through all them in detail. But essentially, we see some imbalances in the gut. There might be Blasto. There might be H. pylori. There is a high probability of some type of yeast.
So, what do we do? Well, the impression that I have in looking at all this is today’s labs show SIBO, yeast, and potentially Blasto. Also, managed autoimmune thyroid—I should probably cue you in that her thyroid, her TPO antibodies came back at 45, so absolutely an acceptable level. But her T4, free and total, were low, okay. So continuing here. So, today’s labs show SIBO, yeast, potentially Blasto and managed autoimmune thyroid. She’s been treated for SIBO, Blasto, and yeast one time in the past and was minimally responsive.
Antimicrobial Protocol
Today, we’ll start with her antimicrobials plus artemisinin plus anti-biofilm agent. So now were taking the antimicrobial protocol and we’re stepping it up a level adding artemisinin, which is a strong anti-Blasto agent and anti-biofilm agents, which can help with the resistant cases. Then we’ll also increase the dose of her probiotics. She had previously been using the lower end of the dose range. But now that we this dysbiosis and knowing that probiotics can be synergistic with the treatment of dysbiosis, we want to turn that up a little bit also. She has responded very well to the paleo/low FODMAP diet and mildly to the initial program. She has recently been diagnosed with PCOS, but luckily her female hormones were in normal levels when tested by her obstetrician. It was just that the ultrasound found polycysts on the ovaries. Okay. And so the OB started her on progesterone. So we’ll continue to monitor her female hormone symptoms and evaluate if the herbal hormone support is helping or not helping, because she has kind of two things happening conjunctively here.
So, my recommendations: maintain the previous program plus start on the following: You can bring the coffee back in. She was happy about that. And we’re going to start on the antimicrobial protocol and layout the exact protocol in the write up along with anti-biofilm agents and artemisinin. Start on the full dose of your probiotics and follow-up in five weeks.
Okay. So when we follow up, about four or five weeks later, she had remarked that the antimicrobial protocol was very helpful. And the progesterone she was taking from her OB also was helpful. She had started cycling. And the mag citrate that we had given her for her bowels was also helping. She also noticed she is more alcohol tolerant. And you’ll see that as you clean up someone’s gut because the gut drains into the liver. And so if the gut is a mess, if there’s a lot for the liver to clean up, once you start improving ones gut health, there’s less taxing stimuli or load on the liver, and so people can be more alcohol tolerant. So, improved were her bloating, distention, body weight, mental fog, constipation, and also some of her female symptoms like her skin, her PMS and her trouble with cycling. And none of her symptoms were non-responsive and none of her symptoms were worse.
 So, my impression, Kaitlyn has responded very well to two months of antimicrobials plus artemisinin plus antibiofilms, along with some mag citrate and progesterone prescription. No further improvement is needed today. So, we will maintain the current plan and then follow up in two months and move, first, to perform a dietary reintroduction and then to reduce the items in her program. Today, we will also take her off the herbal estrogen and progesterone since—and she reported this after the fact she had come off of those with no changes.
So, my impression, Kaitlyn has responded very well to two months of antimicrobials plus artemisinin plus antibiofilms, along with some mag citrate and progesterone prescription. No further improvement is needed today. So, we will maintain the current plan and then follow up in two months and move, first, to perform a dietary reintroduction and then to reduce the items in her program. Today, we will also take her off the herbal estrogen and progesterone since—and she reported this after the fact she had come off of those with no changes.
She was confused when she started the prescription progesterone and she wasn’t sure what to do so came off the herbals. And since she came off those and her female hormones seem to be improving, we just kept her on the progesterone. And I made a note that we’ll consider retesting previous findings at her follow up like the low T4 and the TPO. But I say consider specifically because I don’t feel that it’s essential. So the recommendations and summary: Maintain your previous plans, stop the herbal female supports, follow up in two months.
So, two months later, she has been doing great and has improved even more since her last visit. And she had also noticed that some gas has returned when eating off-plan foods like highly processed foods and beer. And so, that isn’t really highly abnormal, have a little gas if you’re having a slice of pizza and a beer, especially this early on than the healing process. I would anticipate just with time, she’ll probably have an increased resilience there. So, improved were essentially all of her symptoms still except for bloating and distention if she eats a significantly off-plan meal like processed food and beer.
So, my impression: Today, Kaitlyn has continued to improve. She does notice some bloating when eating off-plan foods occasionally. No further improvement is needed today. Today, we will have her perform dietary reintroduction followed by a program curtail. And we will not retest since she was doing so well. Follow up as needed or once yearly. Some of my recommendations and summary: First, perform the dietary reintroduction and then try to reduce your program. Try to find the minimal dose needed of the items in your program. Follow up as needed or once yearly for a check in.
So, I also have two paragraphs here that are essentially my summary. But her case was a good case illustrating that you can see some noise on the thyroid. And that noise doesn’t necessarily require remedying. All of her symptoms were gone. And I’m re-assuming if we retested her thyroid, that her low T4 would have now be normal. But even if her low T4 wasn’t normal, I’m not sure that we would need to act on that in any way because she was perfectly healthy. Her thyroid antibodies were healthy. All of her symptoms were gone. She just required a combination of a more potent herbal antimicrobial protocol combining that with diet and combining that with probiotics.
Now, here’s where some typical misses will occur. You have SIBO, don’t take probiotics, that’s an erroneous recommendation. Will everyone with SIBO benefit from probiotics? No. But do we clearly have data showing that probiotics can decontaminate the small bowel of SIBO? Yes. Do we also have evidence showing that probiotics can help with the clearance of things like H. pylori, Blasto, and yeast? Yes. So it would be foolish not to use these. So we use those in combination with diet, in combination with a stronger herbal anti-microbial protocol and some female hormone support. And that was all it was needed to get her to a point where she was feeling better than she had felt in years. All of her symptoms were gone.
 We didn’t have to do this torturous testing. We didn’t have to do repeat rounds of retesting. So, in a lot of cases, these situations are not that hard to get out of if you have the appropriate model and the appropriate way of navigating these things. So, in her case, she had not done great previously because she had really had just monotherapeutic drug treatments with some strong antibiotics. Which I have no quarrel with those antibiotics per se or in and of themselves, but they weren’t used in a more holistic approach looking at her body holistically and trying to figure out how do we get her back to a more healthy position. We also didn’t get pulled into trying to custom modulate her levels of thyroid hormone. Her thyroid seemed to be generally functioning okay. But it was likely her female hormones, which do have a facilitatory impact on thyroid and her gut, which we know has an impact on thyroid, that needed to be addressed to fix her thyroid. So, that’s another key point is that we don’t want to get always get pulled in the thyroid. There are some cases, I would argue, a good majority of cases where it’s actually the gut that’s driving a problem in the thyroid.
We didn’t have to do this torturous testing. We didn’t have to do repeat rounds of retesting. So, in a lot of cases, these situations are not that hard to get out of if you have the appropriate model and the appropriate way of navigating these things. So, in her case, she had not done great previously because she had really had just monotherapeutic drug treatments with some strong antibiotics. Which I have no quarrel with those antibiotics per se or in and of themselves, but they weren’t used in a more holistic approach looking at her body holistically and trying to figure out how do we get her back to a more healthy position. We also didn’t get pulled into trying to custom modulate her levels of thyroid hormone. Her thyroid seemed to be generally functioning okay. But it was likely her female hormones, which do have a facilitatory impact on thyroid and her gut, which we know has an impact on thyroid, that needed to be addressed to fix her thyroid. So, that’s another key point is that we don’t want to get always get pulled in the thyroid. There are some cases, I would argue, a good majority of cases where it’s actually the gut that’s driving a problem in the thyroid.
And so that’s a case study again from the February 2018 issue of the Future of Functional Medicine Review. If you haven’t checked it out, I would highly encourage you to sign up for your first month of access. It only costs you $1. If you sign up in the month of September, you’ll have your first month of all access for $1 and you can read through all of the—one case study a month for almost two years, all of these research study reviews. There’s a ton of information there. And I think you’ll get a lot out of it.
And I’m trying to make it really easy for you to jump in, have a look around. And if you feel that it’s valuable, I hope you’ll retain your membership. And if it doesn’t seem to benefit you, then no problem at all. It’s just wanting to make it easy for you to be able to read through some of this stuff, learn. And either if you’re a clinician or even a layperson who really wants to be at the cutting edge of this, this is my attempt to really provide you with high quality information to hopefully anchor you amidst the litany of what I sometimes feel to be questionable recommendations made in the functional medicine field; all be it, I think, they’re all well intention.
Episode Wrap Up
So, let me know what you guys think. If you have any feedback, I’m curious to hear it. And this is another episode of Dr. Ruscio Radio. I will talk to you guys next time.
What do you think? I would like to hear your thoughts or experience with this.
- Get help with fixing your thyroid.
- Get your personalized plan for optimizing your gut health with my new book.
- Healthcare providers looking to sharpen their clinical skills, check out the Future of Functional Medicine Review Clinical Newsletter.
Dr. Ruscio is your leading functional and integrative doctor specializing in gut related disorders such as SIBO, leaky gut, Celiac, IBS and in thyroid disorders such as hypothyroid and hyperthyroid. For more information on how to become a patient, please contact our office. Serving the San Francisco bay area and distance patients via phone and Skype.
Discussion
I care about answering your questions and sharing my knowledge with you. Leave a comment or connect with me on social media asking any health question you may have and I just might incorporate it into our next listener questions podcast episode just for you!