Testing & The Gut-Autoimmune Connection with Dr. David Brady
Written by ![]() Dr. Michael Ruscio, DC on
November 7, 2018
Dr. Michael Ruscio, DC on
November 7, 2018
Your gut contains the highest density of immune cells in your entire body, so gut health is very import for those looking to prevent or treat autoimmune conditions. Today we discuss ways to test for imbalances in the gut that may contribute to autoimmunity, including leaky gut and bacterial imbalances.
Episode Intro
Dr. Michael Ruscio, DC: Hey, everyone. Welcome to Dr. Ruscio Radio. This is Dr. Ruscio. Today, I’m here with Dr. David Brady. And Dr. David Brady, not to date you, but when I was a student, I remember your lectures were one of the top lectures I was going to. And it’s funny. Just a snot-nosed student learning from someone, and now being able to have a conversation as peers.
So you’ve been in the game for a while. And you’ve been really a prominent figure in the educational aspect of functional medicine. So it’s great to have you here.
[Continue reading below]
Dr. R’s Fast Facts Summary
What Causes Autoimmunity (AI)?
- Genetics + antigens + gut
- Susceptibility to overreact to things in their environment
- Early life environment: hygiene, breastfeeding, cesarean birth
- Exogenous antigens (Outside environment)
- Gut (leaky gut, microbes)
- Immune system generally reacts to proteins, amino acids, peptides
- Susceptibility to overreact to things in their environment
GI connection to AI
- What to look at … high level:
- Gut microbiota composition: What makes up the gut microbiota?
- First look for pathogens
- Then look at other “opportunistic” microbes that can overgrow (IBS, SIBO, etc.)
- Gut barrier function: How well are you being protected from microbes?
- Leaky gut
- Inflammation
- Pancreatic enzymes, blood in stool, etc.
- Gut microbiota composition: What makes up the gut microbiota?
Dr. Ruscio’s Treatment Hierarchy
- Diet + lifestyle
- Pathogens + symptoms
- Fine tuning – testing: opportunists + commensals, inflammation, leaky gut….
Dr. Brady’s Hierarchy
- Diet + lifestyle
- Pathogens + symptoms + testing
GI-Autoimmune, GI Map and Problematic bugs
- Higher amounts of benign E. coli, proteus, H. pylori are associated with higher levels of AI as well as certain viruses like epstein barr, cytomegalovirus (association does not always = causation)
- Specific by AI disorder and associated organisms
- Autoimmune arthritides
- Klebsiella, citrobacter, proteus mirabilis, prevotella,
- Systemic sclerosis
- Fusobacterium
- Crohn’s and psoriasis
- Mycobacterium
- Autoimmune Thyroiditis (Hashimoto’s and Graves Disease)
- Yersinia enterocolitica
- PANDAS
- Streptococcus
- Chlamydia
- Salmonella
- Reactive Arthritis
- Yersinia
- Guillain-Barre Syndrome
- Campylobacter
- Autoimmune arthritides
- H. pylori
- Optimization strategies aimed to increase the efficacy of H. pylori eradication therapies.
- Helicobacter pylori CagA antibodies and thyroid function in latent autoimmune diabetes in adults.
- This study found that only the virulent strain of H. pylori (identified with CagA) correlated with autoimmunity
GI-Map testing
- *Should be used on context of patient*
- Consider family history, patient history, current symptoms
- The GI Map has good insurance coverage
- False positives – very little
Learn More
- For more about GI MAP testing visit diagnosticsolutionslab.com
- For more about education, chronic pain, and fibromyalgia visit Drdavidbrady.com
- Get the book: The Fibro Fix by Dr. David Brady
- Get help with GI testing.
- Get your personalized plan for optimizing your gut health with my new book.
- Healthcare providers looking to sharpen their clinical skills, check out the Future of Functional Medicine Review Clinical Newsletter.

Subscribe:
Download Episode (Right click on link and ‘Save As’)
DrDB: Well, thank you. Maybe that means that you’ve been doing this long enough now yourself that you’ll know whenever I say something that’s not correct.
DrMR: Well, I think you stay pretty close to the evidence. So I think we have a small probability of that happening. And you’ve been on the podcast before. We talked about The Fibro Fix, your book on fibromyalgia. But in case people didn’t catch that episode, can you briefly give people your background?
DrDB: Well, yeah. I guess I’ve been doing functional, integrative medicine for, I guess it’s 27 years now. And I was trained initially in physical medicine as a chiropractic physician, then went on to graduate nutrition training, and then went to naturopathic medical school and functional medicine training along the way.
So it’s really a mix of a lot of different approaches and backgrounds that, I think, flavor how I approach complex, chronic disease mainly, which is what I deal with in my practice and also in my developmental laboratory testing and nutraceuticals.
And two big focuses of mine in my career have been, one, the whole global pain and fatigue disorder bucket which fibromyalgia is certainly squarely in that. So I’ve done a lot of work clinically but also academically in that realm.
 So you mentioned my latest popular book is The Fibro Fix. And it gives patients a lot of solutions and road maps toward getting the right kind of care and the right kind of diagnosis which is even more important initially.
So you mentioned my latest popular book is The Fibro Fix. And it gives patients a lot of solutions and road maps toward getting the right kind of care and the right kind of diagnosis which is even more important initially.
And then the other big focus of mine in my career, it seems, has fallen into this realm of autoimmune disease. And we have an epidemic going on in autoimmunity as most know. Right now, I think one out of two Americans suffer from some level of autoimmune disorder, which is staggering to think of.
But the increase in the epidemiology and the incidence of autoimmune disorders over the last 100 years and particularly over the last 50 years in the western, industrialized countries is really quite remarkable, quite staggering. And it is somewhat baffling and concerning to public health people and to clinicians alike because we’re dealing with this in our offices day in and day out.
And the solutions that the patients are being presented in the conventional routes of care, although they have their place and they can be effective in symptom management, have a big downside as well with side effects that are serious and not really getting to the root cause of the problem.
So that leaves a lot of people seeking deeper solutions and other avenues of care. And therefore, a lot of them end up in my office. And it’s been quite a learning experience to work with them in their quest to try to get well.
DrMR: That’s a great segue into the topic for today, which will be essentially autoimmunity. And we’re certainly going to flavor this through the perspective of the gut. But we won’t limit it to that. But that’s definitely where I’d like to focus us. And obviously, that’s a fairly prominent area of invention.
David, what do you see as some of the foundational factors that contribute to autoimmunity? And just for the audience in case you’re not familiar with what autoimmunity is, it’s essentially when your immune cells attack normal tissue of your body that they should not. So in something like irritable bowel disease, you attack various aspects of either the gut microbiota itself or the lining of the gut. In rheumatoid arthritis, you attack the tissue. Multiple sclerosis, neurological. Certain skin conditions, although some of these are debatable as to whether or not they’re actually autoimmune or not like eczema and psoriasis, you attack skin tissue. So it’s when the immune system, your internal army, is attacking healthy tissue that it should not.
And there are a number of factors. But let’s, I guess, start, David, with what you consider the foundational factors like environment, maybe early life factors. And then we can work our way to more day-to-day factors.
Autoimmunity Foundations
DrDB: Yeah. Well, that’s a good description for the audience of autoimmunity. Essentially, one’s own immune response, which is supposed to protect us mainly against infection and pathogens, goes off the rails a little bit and gets a little bit confused.
And it loses the ability to differentiate or discriminate between something it should attack and something it should leave alone. And what it should leave alone is our own body tissues. And it should attack things like viruses, bacteria, and other things that could be a threat.
And we have this epidemic, like we said, of people’s immune systems really not behaving normally or optimally. And if you don’t believe me, just walk through an elementary school or a middle school. I have still have children who are in elementary and middle school. And it astounds me, even knowing what I know, when I walk through their schools because every single classroom has a warning sign. “Child with peanut allergy.” “Child with this sensitivity or this or that.”
And it struck me one day that there were none of those signs when I was going to school. And is it just that we didn’t appreciate it, didn’t understand it? Probably some of that. But no, that’s not the answer. The children’s immune systems are really, really behaving abnormally in a much higher prevalence and a much more dramatic way in these current generations. And what has caused all of that? That’s the golden question.
So fundamentally, though, what appears to be the case is to have an immune system that starts going awry and attacking itself you have to have a confluence of events. You have to have a perfect storm, as it would be said, in that the person has to have a susceptibility to overreact to certain things in their environment.
 So there is an inheritable, if you will, genetic risk that people carry. But it doesn’t mean you’re going to have an autoimmune condition. But if you happen to then be subjected to certain triggering substances in the environment, things from the outside, what we would call exogenous antigens (meaning something that’s not within you or normally part of you but something you’re exposed to). If you’re exposed to a trigger that you have a genetic propensity to overreact to, if you will, then you’re laying the groundwork for an autoimmune response.
So there is an inheritable, if you will, genetic risk that people carry. But it doesn’t mean you’re going to have an autoimmune condition. But if you happen to then be subjected to certain triggering substances in the environment, things from the outside, what we would call exogenous antigens (meaning something that’s not within you or normally part of you but something you’re exposed to). If you’re exposed to a trigger that you have a genetic propensity to overreact to, if you will, then you’re laying the groundwork for an autoimmune response.
And what we’re learning is that a third component is that if you have problems in the intestinal environment because we really interact with the most exogenous antigens or environmental triggers through our gut and all the microbes, the bacterium, the viruses, and other types of organisms and the food proteins that are put through the gut. That’s where we interact most with these potentially immune-triggering, outside influences.
And if we have poor health in the gut—and a lot of people, if they go online, will read about things like leaky gut syndrome or intestinal hyper permeability. If those things are present—and we can talk more about why that’s the case. But we know if they are present, that’s a third factor in allowing this perfect storm to come together for your immune system to start picking on one or more of your own tissues.
And those environmental triggers could be in the form of microbes. They often are. So the bacteria that grow in our gut, the viruses that we’re exposed to over time. But it’s not only microbes. It can also be other triggering substances, particularly foods.
The immune system generally reacts to the structure of proteins or amino acids strung together or sometimes if they’re small enough, we call them peptides. That’s what the immune system generally is reacting to. So there are proteins or peptides associated with bacterium, with viruses, but also with the proteins in the food you eat.
There are also proteins that are on your own tissues that are part of you. And sometimes, these proteins can look a lot alike, not exactly alike, but a lot alike. And the immune system can get confused between the subtle differences. It’s almost like two people who look a lot alike. And you lose the ability to discriminate between the faces.
That seems to be what’s happening, particularly with the triggering through a mechanism we call molecular mimicry. So we can talk a little bit more about that. It’s certainly not the only mechanism by which the immune system can be fooled into attacking one of its own tissues. But it’s certainly one of them.
But in the end, we have this confluence of factors. We have a genetically susceptible individual. We have them being exposed to something that they are susceptible to overreact to. And then we have, usually, some sort of level of problems in the gut, particularly with hyper permeability or a leaky state of the gut.
DrMR: Okay. Great. So I was just making a quick note there. And I try to take notes here for our audience as I listen. And sometimes, my fingers can’t move as fast as my brain thinks. Unfortunately, I was not born to be typist.
So I think that’s a great model through which to look at this. And let’s now transition to some of the low hanging fruit. Or maybe “low hanging fruit” is a bad term to use. But what are some of the most relevant facts to look at in the gut that one may want to busy themselves with?
I’m sure you can appreciate this, David, as someone who straddles the line of both academics and clinical practice. There are some things that are academically interesting that don’t really translate to clinical actionables. And that’s one thing I really try to do in the podcast—sift out the academic minutiae and give people, present to people, what are the clinical actionables.
So what do you feel are some of the most relevant factors in the gut one should be looking at as it pertains to autoimmunity?
The Gut and Autoimmunity
DrDB: Well, from a 30,000 foot, big picture scenario, there are two major issues. One is, what is the composition of what we call the GI microbiota? So what is the microbiota? It’s the germs, the bugs, the microbes that live in your gut. And they could be bacteria. They could be viruses, protozoa, larger parasites like helminthes. And there are fungi. There are all kinds of stuff in your gut.
What makes up that composition? What bugs are there? In what numbers? In what percentages to one another? And are they healthy ones? Are they potentially problematic ones? So who’s living there is number one.
 Number two, how well are you being protected from that population of microbes and from the foods that you’re eating before they’re properly digested and pulled apart and rendered less problematic and the toxins that are in the food you eat. How well protected are you from that environment of your gut?
Number two, how well are you being protected from that population of microbes and from the foods that you’re eating before they’re properly digested and pulled apart and rendered less problematic and the toxins that are in the food you eat. How well protected are you from that environment of your gut?
And that comes down to the lining of the gut or the GI mucosa. And that’s where the issue of leaky gut/hyper permeability comes from. And we know that if you have inflammation along the gut lining, whether from infection, from the wrong kind of microbes being there, from the use of nonsteroidal anti-inflammatories and other medications including antibiotics, that a lot of this stuff can get disrupted. Stress can disrupt it. Alcohol, a lot of the modern, processed convenience foods. So there are a lot of factors working not in our favor in the modern, western lifestyle and diet as far as gut health goes.
But as gut health goes bad, whether the wrong kinds of microbes there or the hyper permeability or degradation of the lining of the gut or, in many cases, in most cases of autoimmunity, both things going on simultaneously, then you have the recipe for a big problem.
So what we do from a, like you said, clinically actionable standpoint is to look at that GI environment. So we look at the composition of the various microbes that are there. And we look for ones that we would consider to be beneficial. They’re good. We look for ones that are definitely not good. These are known as pathogens because if they are there in high enough levels, they usually cause overt symptoms like diarrhea or colitis or something.
But then we have a whole bunch of organisms that are not overtly good. They’re not overly bad. They’re kind of in the middle. They take up a lot of the space in the gut. They’re often referred to as opportunist because if the opportunity is presented to them and the GI environment is presented, they can overgrow. They can over express. And then they can cause problems.
They can generate autoimmune responses. They can cause a lot of vague gastrointestinal symptoms like gas, bloating, constipation, diarrhea, distention. A lot of times, these things would be diagnosed as irritable bowel syndrome (or IBS).
So we’re looking at that composition with an eye toward improving it and nudging it toward a better, more healthful state where there’s better diversity, more richness of the beneficial bacteria and less of the ones that are specifically known to either be associated with or, even more so, directly trigger autoimmune responses either through molecular mimicry or through other mechanisms that we can talk about such as the production of enzymes that can change some of our host proteins in the body. So composition of the microbes we look at very closely.
But then we’re also looking at other issues like, is there inflammation on the gut lining? Is there leakiness along the gut lining? Are you adequately breaking down and digesting your food proteins, adequately enough so that they’re not interpreted as threats or antigens?
So we can look at how much pancreatic enzymes you’re putting out. Is there too much percentage of fat or protein in the stool? Is there blood? Are there enzymes that can be introduced by the resident microbes that can cause other problems such as difficulty in eliminating certain substances from the body that you’re trying to detox?
So with the modern laboratory tools that we have as clinicians, we can really zero in in a much greater, detailed, and meaningful way than we were ever able to before, even 5, 10 years ago, and actually look for things that we can then take action on and improve and change the landscape, change the environment of the gut so that you’re taking away the oxygen from the fire, if you will, of the autoimmune process.
DrMR: Sure. That’s a great narrative. And I’m curious to get your thoughts on this, David, because what I’m starting to see in the field is some practitioners start too zoomed in. And they miss the forest for the trees. We have this wealth of laboratory data, which can be helpful.
However, they skip right to the most advanced level assessments and treatments. And they miss some more of the preliminary treatments and inventions that may actually get the patient to the result that they’re looking for.
And so let me throw this idea out. And then I’d be curious to get points you agree with or also, even more so, points that you disagree with. And I really do encourage that because I think it is healthy, especially for our audience to hear disparate views because no one, I think, has got this absolutely right. So hearing different viewpoints, I think, really enriches the conversation overall.
Dr. Ruscio’s Treatment Hierarchy
The way I wade into this is you have someone who is not feeling well. Let’s say they have thyroid autoimmunity and digestive symptoms, just to paint one scenario. So we start with diet and lifestyle. So instead of going right to testing—and again, this is just my opinion. I’m not saying this is right. But this is the approach I find to be most efficient. We start with some dietary and lifestyle changes. And then we reassess.
Now, could we presume that someone who has IBS and thyroid autoimmunity would test positive for high zonulin or skewing of their various bacterial populations? Yes. Does that mean that we need a test to guide the dietary inventions? I think you could make an argument for that. But I don’t think it’s a very strong argument. I think the most efficient path forward would be starting with diet and lifestyle and then reevaluating. And who knows? You may see IBS clear in a having of the TPO antibodies. That, I think, is probably a point we’ll easily agree on.
Second to that is where we might not have the same framework. But again, I’m very open to hearing your thoughts on this.
 I would then look to detecting known pathogens and then treating the pathogens and looking at someone’s symptomatic improvement to gauge whether or not we’ve seen adequate resolution or not. So let’s say we find H. pylori and Candida. We focus on treating those. And then we reassess. And the reason why I advocate focusing on those is so that we don’t—or maybe said another way, it’s because we know that pathogens will poison the milieu and cause things like inflammation and dysbiosis in the sense that inflammation that can ensue secondary to pathogens can make the environment more favorable for bad guys to grow and poison us for good guys to grow. So if you can get rid of the pathogens, then the community can kind of reset back to equilibrium.
I would then look to detecting known pathogens and then treating the pathogens and looking at someone’s symptomatic improvement to gauge whether or not we’ve seen adequate resolution or not. So let’s say we find H. pylori and Candida. We focus on treating those. And then we reassess. And the reason why I advocate focusing on those is so that we don’t—or maybe said another way, it’s because we know that pathogens will poison the milieu and cause things like inflammation and dysbiosis in the sense that inflammation that can ensue secondary to pathogens can make the environment more favorable for bad guys to grow and poison us for good guys to grow. So if you can get rid of the pathogens, then the community can kind of reset back to equilibrium.
And then the final thing I would do if someone still hasn’t responded after that would then be consider testing that looks at enzymes and ratios so that we can fine tune. And now we can try to look more specifically at inflammation or leaky gut and fine tune our approach.
That’s how I’ve been navigating this. Not saying that that’s right. But I’m wondering what there would you agree with? What there would you maybe modify?
DrDB: Well, I think you’re right in that the biggest leverage point we have as clinicians with patients with health in general but certainly with gut health is dietary modulation. I think what patients are doing as far as the kind of food selections they’re making and the quality of their diet and the composition of it is much more powerful than any pills or potions will ever be, whether they’re drugs, nutrients, botanicals, whatever.
It really does start with diet and eliminating things that are overtly harmful to the gut, whether it’s excess of alcohol, NSAIDs, antibiotic use, tons and tons of stress, whatever. I think you have to start with diet.
From the testing standpoint, the issue of going through that sort of triage, like you mentioned, I understand the logic of it. But the reality with testing now is it’s gotten so comprehensive, so amazing, and so low cost and quick turnaround time that if you’re going to test you’re going to get all the information anyway. You’re not going to really, generally, just check pathogens.
If you do, let’s say, like a molecular stool analysis, you’re going to get pathogens. You’re going to get opportunists. You’re going to get commensals (or beneficial organisms). You’re going to get stool chemistry. So you have the benefit of looking at all of that at one time basically.
And you’re right. If there are overt pathogens there, they really should be addressed first because the body reacts to those pathogens being there. And you’re going to get other forms of dysbiosis in the opportunist and in the beneficial organisms just by virtue of the pathogens being there. And the pathogens will drive inflammation and can drive leaky gut syndrome. It can drive all of that. So you’re going to want to try to get rid of those pathogens.
But along the way of doing that, you often can straighten out the opportunists. And I don’t think you have to pick it apart, in doing it in long sequences of protocols. I think you can kill a bunch of birds with one stone, actually, and be extremely efficient—time efficient, cost efficient—in what you’re doing if you make intelligent use of the latest diagnostics that we have. Not that they’re perfect, but they’re a whole lot better than they used to be.
Sponsored Resources
Let’s talk about one of my favorite tests for digestive health, the GI Map from Diagnostic Solutions, who has helped to make this podcast possible.
![]() Now, if you’ve been reading any of the case studies that I’ve published in The Future of Functional Medicine Review clinical newsletter, you’ve likely seen that this test, the GI Map, is a test I frequently use in my practice.
Now, if you’ve been reading any of the case studies that I’ve published in The Future of Functional Medicine Review clinical newsletter, you’ve likely seen that this test, the GI Map, is a test I frequently use in my practice.
Why? Well, one of my favorite things about this test is it has excellent insurance coverage. So this is a few hundred dollars I save patients. This lab is also CLIA certified, which is essentially the quality assurance bureau for labs. So it’s important that these labs are being monitored and not cutting any corners. That’s where you get your CLIA certification.
Now, this test uses quantitative PCR technology. So it’s a DNA test. And you’ll get a good read on dysbiosis with this test because they will assess and report out various types of bacteria, yeast, and parasites including protozoa, worms, and amoebae.
They also have some valuable and helpful clinical markers like calprotectin, which can help rule in or out irritable bowel disease, and zonulin, a marker of leaky gut.
So head over to DiagnosticSolutionsLab.com to learn more and to order your test.
GI MAP Testing
DrMR: Okay. The GI Map, I know, is a test that you’ve been aiding in the development. And I believe you sit on their advisory board on some capacity to help connect the science to the lab. So I know that you’re at the forefront of the research here.
What do you feel are some of the more well-studied organisms that associate or, even better yet, have shown to be causal to autoimmunity? And I’ll just throw out a couple.
I think H. pylori is probably the most advanced where there’s a lot of association data, and there’s a handful of cause data. And when I say “cause,” I’m inferring that from treating H. pylori showing subsequent improvement in autoimmunity. I think that may be the most well developed. But there could be some things I’m missing there.
SIBO, there’s some exciting association data. And then also Yersinia and Epstein-Barr virus, there’s, again, mostly association data. And then the helminthes is actually a wild card which seems like it can cut either way.
But get us up to speed on what we know and where we should be looking.
DrDB: Well, if you’re looking at which organisms themselves have been correlated, like you said, through association data, which means more of those organisms present are associated with a higher incidence of autoimmunity in general or in some cases a higher incidence of a specific autoimmune disorder, that’s pretty well established across a long list of organisms.
But a caveat to that, like you alluded to, is association does not mean causality. Does it mean just because it’s there, you will get autoimmune disease X? It means there’s a higher risk of it. But then again, you have to be that genetically susceptible individual and have certain characteristics of your immune response that allow it to overreact to that organism that may be there or other antigens. And you probably also have to have this hyper permeability/leaky gut. So you need a couple of things to gang up you or stack up, if you will.
So just the fact that the organism is there does not mean that you will get it. And in some of these studies, the association may have nothing to do with the autoimmune disease. It’s not necessarily a causal link.
Now, there is other research that shows mechanisms of causation or actual etiology of the genesis of an autoimmune disorder. And we can talk about some of those.
 But back to the answer, organisms like just higher amounts globally of E. coli, even benign E. coli—I’m not talking about Enterohemorrhagic E. coli or any of the bad E. coli associated with food poisoning and things like that. I’m just talking about more E. coli in general, more Proteus in general. You mentioned H. pylori. And of course, these are bacteria. And they’re associated with higher levels of autoimmunity in general. But so are certain viral organisms like Epstein-Barr virus, cytomegalovirus, and many of the so-called ubiquitous viruses.
But back to the answer, organisms like just higher amounts globally of E. coli, even benign E. coli—I’m not talking about Enterohemorrhagic E. coli or any of the bad E. coli associated with food poisoning and things like that. I’m just talking about more E. coli in general, more Proteus in general. You mentioned H. pylori. And of course, these are bacteria. And they’re associated with higher levels of autoimmunity in general. But so are certain viral organisms like Epstein-Barr virus, cytomegalovirus, and many of the so-called ubiquitous viruses.
But when it comes down to getting a little bit more specific by autoimmune disorder, there’s lots of data. Probably the oldest stuff out there is on Klebsiella species, Citrobacter species such as Citrobacter freundii, also Proteus mirabilis, Prevotella.
These are all organisms mainly associated with autoimmune arthritides. So rheumatoid arthritis, ankylosing spondylitis. Fusobacterium in systemic sclerosis or scleroderma. We have Mycobacteria in psoriasis but also in Crohn’s disease. You mentioned Yersinia, in particular Yersinia enterocolitica in autoimmune thyroiditis as like Hashimoto’s and Graves’ Disease. We have Streptococcus and PANDAS in children. And then Chlamydia, Salmonella, Shigella, Yersinia also in reactive arthritis. And on and on. Campylobacter jejuni in Guillain-Barré syndrome. So there are lots of stuff out there.
So we are screening for those specific organisms when we do a GI Map. But we’re contextualizing it. And that’s very important. We’re not just doing a GI Map and looking at results.
We’re doing a GI Map and looking at results in a specific patient that we know what their clinical scenario is. What is their history? Not only their personal history, but what is their family history? That’s very important. And what are they expressing clinically? What is their examination like, maybe what their imaging is like? What are their complaints? It all has to be contextualized.
But I can tell you if I have a GI Map that comes back on, let’s say, an individual in their 20s. They’re fairly healthy. Maybe they had some gut issues or something, some gut complaints. We did a GI Map. And I see that they have a lot of DNA recovery for Klebsiella, for Citrobacter, for Prevotella.
And when I start asking about their family medical history, they tell me, oh, their father had rheumatoid arthritis. Their uncle has rheumatoid arthritis. Well, then, those things really mean something to me.
I need to change that patient’s milieu and landscape. Or else, guess what they’re going to have in the future? It’s pretty clear at that point even without testing HLA patterns and protective autoantibodies, which we can do. But if their family history is littered with autoimmunity, but particularly in this case with autoimmune inflammatory arthridities like RA and they come back with the microbiota signature consistent with RA, they’re on the road to RA unless we change something.
Same thing with, let’s say—I’ve had this scenario play out in my practice more times than I can possibly count. Let’s say a female in her late 20s, early 30s comes in. She’s complaining that she’s gaining weight. She can’t maintain body composition like she used to. She’s tired all the time. She’s constipated. She has IBS.
And when we do her exam, her temperature is low. She says that she’s always turning up the thermometer when everyone else is turning it down. Her hair and skin are dry. Her hair is falling out. All of that.
I do her family history. Her mother is on Synthroid. Her older sister is on Synthroid. And we do something like a GI Map. And she comes back full of Klebsiella or Epstein-Barr virus or cytomegalovirus. She’s on the road to an autoimmune thyroiditis. She’s probably a Hashimoto’s disease waiting to happen.
 And then when we drill down deep into their thyroid hormone fractions and their thyroid peripheral metabolism, there are major, major problems going on, oftentimes flying under the radar of their conventional family physician or even endocrinologist because their TSHs aren’t sky high yet. And even their T4, if they measure that, is not entirely out of the normal reference range. But when we look at their levels of T4 versus their T3, free T3 versus reverse T3 and all of that kind of stuff, there are a lot of problems brewing.
And then when we drill down deep into their thyroid hormone fractions and their thyroid peripheral metabolism, there are major, major problems going on, oftentimes flying under the radar of their conventional family physician or even endocrinologist because their TSHs aren’t sky high yet. And even their T4, if they measure that, is not entirely out of the normal reference range. But when we look at their levels of T4 versus their T3, free T3 versus reverse T3 and all of that kind of stuff, there are a lot of problems brewing.
But they’ve never been diagnosed as a patient with a thyroid issue. But we can pick that up very, very early. And we can actually be predictive that, if nothing changes—if you don’t change anything in this patient, they will eventually get to the point where they’ll be diagnosed with an autoimmune hypothyroidism eventually, even by a conventional endocrinologist or their family physician because the train is rolling down the tracks. And they’re basically starting to pick on their own thyroid tissue, pulling it apart a little bit over time. And eventually, they’ll get to the point where they cannot maintain even the semblance of normal thyroid function.
DrMR: I’m glad you made the note about context being important because there is this double-edged sword that we wield which is, one, having this progressive data. But the other is not making everyone who has any abnormality fearful that they’re a ticking time bomb.
And this is the other side of the conversation that I just want to quickly touch on to help anchor and ground people. Make sure you’re looking at these in the context, as David very aptly put, of your family history, your own history, your current symptoms, and whatever other context the clinician may be looking at. Those are just a few things to consider.
So that you can act appropriately but also not overreact because that’s something I’ve seen and I’m seeing as a growing problem. It’s almost like it reminds of this saying from Martin Luther King. “We have guided missiles but misguided men.” Our technology is getting maybe outpaced for how to interpret and utilize that technology responsibly in some cases. That’s at least what I’m seeing sometimes. David, are you seeing this at all yourself?
DrDB: I agree with that. But I also acknowledge it’s a double-edged sword. We also don’t want to ignore the tremendous technology and predictive value that we have in it because it’s being generally ignored in conventional clinical medicine. The research is incredibly advanced. But it’s not trickling down into everyday medicine.
I’ll give you an example. If we have a patient that comes in and they don’t have any joint pain. They have no anatomical derangement of any joints. There’s no swelling. There is no redness. There’s no loss of motion, anything like that. But their family history has, let’s say, rheumatoid arthritis in it. And we do some testing. Let’s say we do GI Map. And they have some of those organisms we talked about associated with RA. Let’s Prevotella, Proteus, Citrobacter, something like that.
But then we turn to the laboratory and do some blood work on them. And their HLA-B27 positive which means they have some of the genetic risk for rheumatoid arthritis. And then if we turn to more predictive antibody types of tests. Let’s say we look at rheumatoid factor. And we look at another one called anti-cyclic citrullinated peptide (or ACCP, some doctors just say CCP). This is an incredible marker. And it can be high years, many, many years, 10 years, 15 years in someone who is on the road to getting RA before they actually have any signs or clinical symptoms of RA that a doctor would cue up and consider or diagnose as RA.
 So do we want to ignore the technology and the opportunity to find out, “Hey, this is a person who will eventually have all of the overt signs and symptoms of RA, will eventually get diagnosed in 10 years.” By then, the opportunities to turn the tide or stop the train from barreling down the track to more joint destruction has been lost to some degree. And their only option then is response modifiers, strong immune suppressors and things like that control the symptoms and the overt joint destruction.
So do we want to ignore the technology and the opportunity to find out, “Hey, this is a person who will eventually have all of the overt signs and symptoms of RA, will eventually get diagnosed in 10 years.” By then, the opportunities to turn the tide or stop the train from barreling down the track to more joint destruction has been lost to some degree. And their only option then is response modifiers, strong immune suppressors and things like that control the symptoms and the overt joint destruction.
Where, if we did that kind of testing now, we can change the equation. We can change their diet. We can improve their gut function. We can get rid of some of these triggering organisms from their GI microbiota. We can help them fix the leaky gut syndrome. We can basically change their lifestyle in a way that has an impact to where they don’t progress and eventually develop that disease.
Now, is it being too proactive to do that kind of testing? Not if the family history dictates that you should.
DrMR: Yeah, no. I agree with you 100% there. And I’m glad you made those clarifying remarks. And this is what I think is responsible medicine where it’s building a case. And I think it’s an excellent way of looking at this. And that’s exactly what I mean by looking at these contextual factors.
DrDB: Let me give you an example of that. Now I brought up that CCP test (anti-cylic citrullinated peptide). Well, what is that? Now, doctors learn that in medical school. They learn—you have someone in front of you. They have some clinical signs and symptoms of rheumatoid arthritis, and you think that’s what it is. Well, to confirm the diagnosis, maybe you do a rheumatoid factor or an ACCP. And it comes back positive. Voila!
But that’s being used in the wrong way, in my opinion. You’re using it to confirm a diagnosis once it’s clinically apparent. What they should be using these tests for instead is in a predictive manner.
So they should be doing these in people with family histories of these disorders because these markers can be positive, like I said, 10 or 15 years before you’d ever think to order it to confirm a diagnosis that you see clinically.
And that ACCP test is revolving around a phenomenon that involves gut bacteria or oral bacteria. For instance, the organism that causes more periodontitis or gum disease or gum infection than any other is P. gingivalis. The organism P. gingivalis, when it overgrows in the mouth, causes gum disease and poor dentition and things like that. It also produces, as a metabolite for its own use and it excretes it, an enzyme called PAD4.
And what PAD4 is used for in the organism is to modify some of the proteins that the organism needs for its metabolism. And it swaps an amino acid on a protein. And when it excretes that enzymes, it can actually modify and effect the person who is infected with that organism’s protein.
So it actually modifies collagen, vimentin, fibrinogen, all these proteins that are associated with joint structure. And it takes an arginine off the protein, one of the amino acids, and it replaces it with a citrulline. So that’s why it’s called anti-citrullinated peptide.
So the lab test is looking for the fact that that phenomena occurred, that the enzyme was produced. It modified your protein. And now that you modify one of your proteins, the structure is slightly different than what it should be. And your immune system now looks at this protein—it might be your collagen, your fibrinogen, your vimentin that’s making up structures in your body. And it says, “Hey, that doesn’t look like me. I’m going to attack it.”
And that’s how the autoimmune process starts. And that’s not association data. This is an overgrowth of a bacterium. So it’s part of our microbiome (in this case, in the mouth), producing an enzyme which modifies our own proteins which makes our immune system now not look at it as us, makes it attack it and destroy it. And it can lead to clinical rheumatoid arthritis. This isn’t association. This is causal.
Now, it’s not the only cause for rheumatoid arthritis. That’s the thing that doctors have to start thinking about. Their old way of being trained in old, acute, infectious disease medicine when Koch’s postulates and the “one organism, one disease, one cause, one outcome” needs to be radically changed. We need to rewrite the medical textbook.
We have the first book of medicine which is acute, infectious care medicine. That’s what western medicine is incredibly good at. But what they’re dropping the ball at, frankly and not managing well is complex, chronic, metabolic disease. That’s because it requires a whole different textbook and a whole different way of thinking because the insult is long gone. It’s what the body is doing long term, stuck in a loop. That’s a destructive process. Because of maybe an insult a long time ago, you have to look at those things differently.
And it’s not one reason, one cause getting you to the same place. There’s a multitude of different potential triggers for autoimmune conditions like RA or diabetes or whatever it may be. So we have to think in a much broader way.
But doctors being trained right now, they’re trained to order an ACCP test in the lab to confirm rheumatoid arthritis. And if you ask those doctors, “What is an ACCP test? Why do we test that?” They have no idea. They just know, “That’s a test I do to confirm RA.” They don’t know why the test exists, what mechanisms it’s based on. And if they knew, they would probably be blown away that it goes back to the microbiome and organisms modifying host proteins.
So it’s really a test that is resonant with functional medicine doctors, integrative medicine doctors more so than conventional docs even though they use the test all the time.
H. Pylori
DrMR: And along those same lines, there’s another facet of H. pylori, I guess, fine tuning testing that some utility seems to be emerging. And this is something I think has been evolving in the body of literature for a while now. And we’re starting to see greater confirmation being published, which is that not every type of H. pylori is as virulent or as detrimental as others.
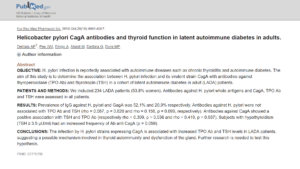 And it’s the CagA type that tends to be more virulent. I’ll put a link in here to a study that found that it wasn’t an association between H. pylori specifically that had a direct correlation to increasing TSH and increasing thyroid autoimmunity. It was only the CagA type or strain of H. pylori that was shown to have that virulence.
And it’s the CagA type that tends to be more virulent. I’ll put a link in here to a study that found that it wasn’t an association between H. pylori specifically that had a direct correlation to increasing TSH and increasing thyroid autoimmunity. It was only the CagA type or strain of H. pylori that was shown to have that virulence.
And this is one of the things that I think is nice about the additional window we can get into with the GI Map testing. And I put this actually in one of our more recent newsletters, that if clinicians wanted to get this deeper assessment into it, I know that this is one of the things that the GI Map offers. So while we’re on the topic of the GI Map, I think that’s worthwhile to mention.
DrDB: Yeah, that is an interesting thing. When H. pylori was first identified as this bacterium or organism that can be causal or the genesis of gastritis, duodenitis, ulceration in the upper GI mucosa, things like that, well, then it was a knee jerk reaction. “H. pylori is bad. It’s a bad actor. Whenever it’s there, we’ve got to eradicate it.”
Well, that’s not necessarily true. We know that people who have more H. pylori have less atopic disorders. They have less asthma and eczema and things like that. It is an organism that there’s ying and yang to, like most.
And it’s not just, “Do you have H. pylori present?” A lot of it is, how much H. pylori? But even more than that, what you said. What are the characteristics of the resident population of H. pylori you have? Do those organisms have the genome or the genetic characteristics to allow them to produce certain chemicals, compounds, or metabolites that actually cause the erosion and the destruction of the GI mucosa? And these are called virulence factors.
When you’re looking with quantitative PCR molecular or DNA technology at these organisms, you can ask questions like, is there more H. pylori DNA being recovered in this patient’s stool analysis than what would be considered normal? Okay. Yes, there is. In that case, do we see the actual genes associated with H. pylori that allow it to make a whole host of different virulence factors?
And on the Diagnostic Solutions Lab GI Map you were talking about, there are, I think, nine virulence factors. Let’s see. One, two, three, four, five, six, seven, eight virulence factors right now, including CagA which you alluded to before. So you can answer the deeper question. Not just, is there H. pylori or not? Or is there more H. pylori or not than the average person? But is it benign H. pylori? Or is it particularly problematic H. pylori?
If you get elevated H. pylori recovery in a patient of yours but they also have three or four or five virulence factor genetic characteristics, then that’s a problematic, highly suspect H. pylori population. And particularly if they have reflux, GERD, things like that, then that’s something that is treatable, in my opinion.
DrMR: One question here, David, which sometimes comes up regarding using PCR testing which is false positives. Do you find false positives with DNA is something that we have to be cautious of and a bit circumspect and making sure to interpret in the context of the patient? Or what are your thoughts there?
DrDB: Well, I don’t think it’s as much false positives as, what is your threshold for considering something significant? If the molecular technology is being done right, there’s very little in the way of false positives. The DNA is there, or it’s not. It matches up to the probe, or it doesn’t.
The question is, is the amount that you’re finding clinically significant in the patient that you’re dealing with? And that’s where you need the skill and experience of the lab to cut their cut points or their thresholds to meaningful levels.
There’s always going to be a level of background, scattered DNA of all kinds of organisms, including overt pathogens, in the food mass that anyone is eating. So when you’re eating food, it’s full of different organisms, when you’re eating it, and their DNA. And many times these organisms are dead. But the DNA is still there.
So if you’re just getting little, little trace amounts of DNA of certain organisms that are transient because of the food that you ate, you don’t want to report those as a positive that needs to be treated medically. So that’s where some of that kind of stuff comes in.
But there was an adjustment period where clinicians—when everything moved to molecular or DNA-based technology versus the old culture technology, it was a learning curve because back in the day in culture technology, it was really hard to find stuff. And the only stuff we were really dealing with was aerobes. Most of the bugs in the gut are anaerobes. So you couldn’t even culture those to begin with.
 Many of the parasites and things like that had to be found under a microscope, on visual inspection, or with some chemical-based tests which were not nearly as sensitive as molecular.
Many of the parasites and things like that had to be found under a microscope, on visual inspection, or with some chemical-based tests which were not nearly as sensitive as molecular.
So it’s almost like doctors all of a sudden put on these magic glasses which let them see orders of magnitude more clearly than they did before. And now they have to get used to seeing a bunch of stuff and deciding whether it’s important or not. So I think we’re still in that learning curve. I think doctors are probably still in a little bit of a state of shock on exactly what is there now that we have the ability to see it.
DrMR: Which I think is a good point to just echo. This is why it’s important to look at labs in the context of the patient. And we don’t want to just take one lab finding and over extrapolate from that. We want to build a case, either to intervene or not intervene, as David outlined earlier. And I think that goes a long way for helping patients get the most out of their testing, to make sure they’re on the progressive cusp but also make sure that they’re not falling over the edge into the zealotry.
View Dr. Ruscio’s Additional Resources
DrMR: David, any final words that you want to leave the audience with or final points that you want to mention? And then also, would you please tell people where they can find out more about you, your work, the GI Map, and anything else that you’d like to mention?
DrDB: Yeah, sure. Well, thank you for the opportunity, first of all, because I think it’s really important to get the word out, not only to my peers, healthcare practitioners, but also to interested people in general, whether they have autoimmune disease or a family member does or whether they’re just trying to be very proactive about their health, that we really do have the ability now. And we have tools. And they’re getting better and better. So 5, 10 years from now, we’ll look at what we have today and think it was rudimentary.
But we have the ability, and in the hands of a skilled physician who can really think their way through this stuff and, like you said, apply it in the right way, to be extremely proactive and predictive about who might go on to develop disorders that, once they fully develop, you’re much more limited in what you can do about them.
Right now, conventional medicine is in the mode of waiting until it happens and then reacting. But these new technologies and the new ability to mine metadata and to understand these different relationships and to collect very personalized information—genomics, microbiomics, metabolomics, proteomics.
“Autoimmunity presents an incredible opportunity in that regard because of the types of predictive testing that we have where we can change people’s fate”![]()
We’re starting to put all these things together in ways that are going to allow us to really develop precision, personalized recommendations for people on things like, what do they eat? What kind of diet should they follow? What kind of nutrients should they maybe potentially take? What botanicals might they respond well to and not? What drugs might they respond to well and not? What kind of movement and exercise and stress management should they utilize as part of their regimen to have the most impactful outcomes on their health?
And autoimmunity presents an incredible opportunity in that regard because of the types of predictive testing that we have where we can change people’s fate. And that really is preventive medicine. Up till now, preventive medicine has been a lot of talk and not a lot of walk. It’s changing rapidly if we utilize the tools.And that’s where we’re going to. And I think it’s going to just blow the lid off upstream lifestyle, nutritional, naturopathic, functional medicine, whatever you want to call it. But we’re going to have lenses into being able to really change people’s outcomes. And I look forward to doing that and helping to push that forward.
But you’re right. We don’t need to over utilize the tools for the wrong reason. So it’s an interesting, brave, new world in this regard. But it presents incredible opportunities.
Episode Wrap Up
So if you want to learn more about the Diagnostic Solutions Lab GI Map test we were talking about, you can just go to DiagnosticSolutionsLab.com. So DiagnosticSolutionsLab.com. And you can learn more about it there. There are some tabs for patient education. And if your provider doesn’t use it yet, you can let them know about it. Share the website with them and so forth.
And then if you want to learn just a little bit more about me and my work, probably two best places to turn are either just my general website, DrDavidBrady.com. And there are all kinds of educational tabs and articles and interviews and different things that you can access there.
But if you have a specific interest in fibromyalgia issues or chronic global pain issues, then you can also check out FibroFix.com.
DrMR: Awesome. Well, David, this has been a great conversation. Thank you again for taking the time.
DrDB: Thanks, Dr. Mike. Appreciate it.
DrMR: You got it.
DrDB: Bye.
- The Fibro Fix, by David Brady
- Helicobacter pylori CagA antibodies and thyroid function in latent autoimmune diabetes in adults.
- Bolus Weekly Vitamin D3 Supplementation Impacts Gut and Airway Microbiota in Adults With Cystic Fibrosis: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial.
- Role of vitamin D on gut microbiota in cystic fibrosis.
- Gut microbiota interactions with the immunomodulatory role of vitamin D in normal individuals.
- Diagnostic Solutions Lab
- DrDavidBrady.com
- FibroFix.com
- Dr. Ruscio’s Additional Resources
What do you think? I would like to hear your thoughts or experience with this.
- Get help using this information to become healthier.
- Get your personalized plan for optimizing your gut health with my new book.
- Healthcare providers looking to sharpen their clinical skills, check out the Future of Functional Medicine Review Clinical Newsletter.
Dr. Ruscio is your leading functional and integrative doctor specializing in gut related disorders such as SIBO, leaky gut, Celiac, IBS and in thyroid disorders such as hypothyroid and hyperthyroid. For more information on how to become a patient, please contact our office. Serving the San Francisco bay area and distance patients via phone and Skype.
Discussion
I care about answering your questions and sharing my knowledge with you. Leave a comment or connect with me on social media asking any health question you may have and I just might incorporate it into our next listener questions podcast episode just for you!