Effective Anti-Aging Treatments for Hair Loss and Skin
Written by ![]() Dr. Michael Ruscio, DC on
March 6, 2019
Dr. Michael Ruscio, DC on
March 6, 2019
When considering your options for anti-aging treatments for skin or hair loss therapy, know that individuals respond differently to different treatments. Together with your doctor, you’ll want to consider the possible causes of your hair loss or skin health to determine the best course of action. Some of the main drugs on the market like Rogaine (minoxidil), which stimulates blood flow to hair follicles, and Propecia (finasteride), an oral dihydrotestosterone (DHT) blocker, are designed to treat the most common cause of hair loss in men and women, androgenetic alopecia. However, causes may not be as clear-cut for all women. PRP injections, dermarolling, low-level light therapy and stem cells offer fairly natural ways to stimulate your body’s own healing responses, for skin rejuvenation and hair loss reversal. No magic bullet exists, but these therapies may also be used in combination, potentially yielding synergistic, better results.
Hair Loss Therapies
- Rogaine
- Finasteride and Dutasteride
- PRP
- Stem Cell
- Hair transplants
- Microneedling
- Root cause – hormones, thyroid, stress
Causes of Hair Loss
- See the infographic below in the transcript
Dermarolling for hair
- Dermarolling is like irrigating your scalp
- For the scalp (.5 to 1.5 millimeters)
- You may need numbing cream
- It can help in combination with PRP or other therapies
- Results appear in 2-3 months
Dermarolling for the face
- For the face (.3 – .5 millimeters)
- Once per week as long as you are not causing too much irritation
- Careful when treating the area around the eyes
Hair loss treatment is a long game
- Best to try several therapies to start, keep an eye on results, then try eliminating some of the therapies to see if you can maintain results
Laser Therapy
- Red light therapy that activates ATP production in mitochondria
- No pain
- No side effects
- No downtime
Laser Device
PRP (platelet rich plasma)
- 3 treatments, one month apart (gain 18-33 new hairs per centimeter)
- Expect to see results after 3-6 months
- Results can last 1-1.5 years
- Some might experience increased hair loss right at first but that is a good sign of starting a new hair cycle
Finasteride
- Helps decrease hair loss with Androgenic Alopecia
- Dosing: 1mg is about as effective as 5mg
- Works for women with Androgenic Alopecia
- Combine it with other therapies for best results
Stem Cells
- Responsible for keeping up cell function
- Taken from fat or bone marrow
Exosomes
- Messengers from stem cells
- Can be used in addition to PRP
Where to learn more
In This Episode
Episode Intro … 00:00:40
Causes of Hair Loss … 00:03:28
Using a Dermaroller for Hair Loss … 00:08:13
Dermarolling for Skin … 00:18:58
Minoxidil for Hair Loss … 00:23:40
Philosophy of Hair Loss Treatment … 00:25:37
Low-Level Light Therapy for Hair Loss … 00:27:29
PRP Injections for Hair Loss & Skin … 00:32:50
Finasteride for Hair Loss, Side Effects … 00:38:28
Stem Cell Therapy for Hair Loss & Skin … 00:48:01
PRP vs. Micro-Needling for Skin … 00:52:53
Episode Wrap-Up … 00:55:52

Subscribe for future episodes



Download this Episode (right click link and ‘Save As’)
Episode Intro
Dr. Michael Ruscio, DC: Hey everyone, welcome to Dr. Ruscio Radio. This is Dr. Ruscio. I’m here with Dr. Amy Killen. And I am really looking forward to this conversation. It’s going to be an exposé on some therapies for hair and skin health. And we were introduced by Tyna Moore who came on and talked about PRP and other injectable therapies for joint health. I was really impressed with her. I said, “We’ve been looking to do a follow-up on this for PRP and like applications for skin and anti-aging, because we get a fair amount of questions about that.”
And she said, “Amy’s the one you’ve got to talk to.” And we had a phone call about a month and a half ago that turned into an hour of me just picking her brain. I wish we recorded that because that was great. But I’m definitely looking forward to digging back into this with you, Amy. So welcome to the show.
Dr. Amy Killen: Thank you for having me.
DrMR: It’s great to have you here. Really quick, give people your background and then we can get into the nitty gritty.
DrAK: Okay, so my background is emergency medicine. Actually I did ER for about 10 years. But for the last six years, I have been focused on integrative medicine and regenerative medicine, using a lot of PRP, stem cells, and therapies to help patients use their own bodies to heal themselves. As well, I use an integrative medicine approach, helping them with diet and exercise, nutrition, supplements, and all those things. So that is what I do full-time now, but I did come from an ER background.
DrMR: So quite the shift there.
DrAK: Yes, two very different fields.

DrMR: Yeah. There’s a lot here in this realm. What would you say is an overview of the main players? PRP is one, of course. There’s also hair lasers. People have probably heard about different hair solutions like minoxidil. There’s stem cell injections, exosome injections, dermarolling (which is something I recently came across). I think we’ll probably hit all of these. Are there any other therapies you think are noteworthy that I left out of that list?
DrAK: For hair, you mean?
DrMR: For hair or for skin.
DrAK: Minoxidil (Rogaine), the main one for hair, is still very effective. It’s listed as an FDA-approved medication. Finasteride and dutasteride, which are prescription medications you can take orally, can also be really effective, if you can handle the potential for side effects.
Then PRP has been pretty well-studied now for hair. It can be quite effective, although it does take several treatments. Stem cells are a bit of a newer player in the game. There is some evidence that they can also be helpful, certainly, but we’re still learning about what types of stem cells and what types of exosomes. And of course, hair transplants are something else that people do. I don’t do that particularly myself.
Causes of Hair Loss
The first thing is actually finding out the reason for the hair loss, investigating things like your hormones, your thyroid, your stress. All those things can play a huge role in hair loss for both men and women.

DrMR: So let’s start with the stress. I’m assuming most people listening probably know enough to have those bases covered with diet, lifestyle, stress, hormones. They’re probably sleeping enough, exercising, eating pretty well. People probably don’t have any major deficiencies, they’ve probably got a lot of stuff sorted out. Also with the hormones, I’m assuming people have been screened for any overt-hypothyroidism, and if there are any women who have pretty raging symptoms of female hormones, I’m assuming they’ve taken steps. So I don’t want to go too into detail there because I think that might be rehashing some stuff for people. But in short, what are some of the more common things that you’re seeing people grapple with in that bucket?
DrAK: There are few things people may not realize. Certainly both low and high thyroid can cause hair loss problems. The most common cause of hair loss for both men and women is androgenic alopecia. That’s this male pattern baldness, associated with dihydrotestosterone production and sensitivity, which is actually the most common cause for men and women. Most men have that. 96% of men who have hair loss have androgenetic alopecia. With women, it’s not quite so simple. So when they have hair loss, we look at the thyroid, we look at things like ferritin levels. Ferritin is your stored iron. A lot of women have low ferritin even though they’re not actually anemic. So we look at trying to get their ferritin up higher, maybe above 80 or so. That’s something people don’t realize can cause hair loss.
I have a lot of women who also don’t get enough protein in their diet. People also don’t realize that not getting enough protein can cause hair loss. Stress can cause hair loss, we know with women especially, also hormonal changes, stressful events, childbirth, even pulling your hair back in a ponytail every day. Finally, we look at medications. There’s quite a long list of medications out there, including things that you wouldn’t even think about, nonsteroidals like your Ibuprofens, other steroids, antifungals. There’s a huge list of medications that can also cause hair loss. So it’s a pretty big list of things we look at, before we even start thinking about the more invasive procedures and such.
DrMR: Now, in terms of medications, are there any fairly common medications? I’m assuming people are trying to take the least amount of any NSAID possible. And if they’re using something like prednisone or a prescription antifungal, hopefully they’re doing that as sparingly as possible. But are there any that are somewhat common and used more in the long term that you think people should consider?
DrAK: Yeah, so statins are associated with hair loss. Beta blockers for blood pressure also cause hair loss, and birth control pills of all different types can. Other things that have been associated include, like I said, the NSAIDs, the prednisone, Pepcid, even some of the H2 blockers, some anticonvulsants, some of the antidepressants, Coumadin, Accutane. There are really quite a number of medications that can be associated with it. Obviously I would never tell a patient to stop taking their medications. But if they’re having new hair loss that’s timed with the medication, then we at least look at that as being a potential contributor.

DrMR: Sure. To your nod on ferritin, I don’t know if we’ve discussed this in the podcast. I don’t want to over-extrapolate, but there was one study recently looking at hypothyroid women who were on medication, yet had non- or poorly responsive fatigue. They found an association to low ferritin (defining low ferritin as ferritin below 100). I believe they found that those women showed improvement with iron supplementation. At very least, they correlated ferritin below 100 to fatigue.
DrAK: Mm-hmm.
DrMR: I do think there’s something to be said for ferritin. We have to be careful, because ferritin can cut the other way too if it’s too high. But I do think there’s something to be said for a nuanced look at ferritin.
DrAK: Yeah. It’s an acute phase reactant obviously. I see a lot of men who have really high ferritin, and that’s something that you would worry about, looking for the reason for that. But for women especially, I see low ferritin. Also patients that are vegan and patients who are vegetarian sometimes, who just are not looking very closely at their iron intake and animal protein intake.
Using a Dermaroller for Hair Loss
DrMR: Right. So, let’s start with dermarolling. If you disagree with me, please let me know, because clearly you’re the expert here. But a dermaroller, for the audience, is this little roller of needles that, as I understand it, causes these little micro-abrasions that help to stimulate circulation and collagen production. Amy, please fill this in, correctly, when I get done with my rant here–
DrAK: Yeah, I love it, haha.

DrMR: But I recently came across one study about men who were non- or poorly-responsive to topical Rogaine (minoxidil), who started doing dermarolling once a week. So you just roll this little pin-roller on your head on a few different areas or in a few different directions. You do this once a week for the first four weeks, I believe. Then for the next two months after that, they did it once every other week, and this group of men showed a significant improvement in hair loss. I believe it would also work for women, but I don’t think it’s been studied.
Dermarollers are 20 to maybe 50-ish dollars. And this is something you could do at home on your own, cheaply, once a week. This to me was pretty cool. It’s almost like a hormetic stressor, right? It’s like one of these stressors that’s a little bit noxious. It irritates and stresses your muscles, but then they recover stronger and more robust. So, I think this may be a cheap, easy intervention that people can start with and may have some pretty cool applications to studies in hair. I don’t know anything about its application in skin. But Amy, very curious to hear what you think about dermarolling.
DrAK: Yeah. I will say that in the studies that I’m aware of for hair—the two that I know of or maybe even three—they use a dermaroller that was one and a half millimeters. That’s pretty deep. As far as I know, you can’t buy a 1.5 millimeter dermaroller over the counter.
DrMR: You can. I bought one on Amazon right after I read the study.
DrAK: You can? Did you get one?
DrMR: Yeah, I haven’t used it yet.
DrAK: Good luck using it. You might want to get some topical numbing cream. The scalp is very sensitive and I know from experience with myself and patients, that one and a half millimeters on the scalp could be painful. You just keep it in mind. You grin and bear it, or get some numbing cream which you can get over the counter and in lower concentrations. Yeah, so it looks like once a week. And then in these studies they were doing minoxidil applications twice a day as well, which is something important to point out.
But the dermarolling, even by itself, could have utility. I use it with PRP, because I want to get the PRP deeper into the skin and into the hair. By dermarolling we’re creating these little micro-channels. So we’re punching these little tiny holes all over the skin and hair, and it’s a great way to induce collagen production just from the mechanical stress. But it also allows me to get the PRP deeper into the skin than I’d able to get it just by putting it on the skin topically.
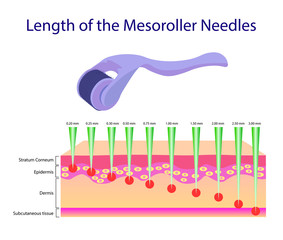
DrMR: Right. So would you recommend a 0.5 or a one in length? Is that what we’re looking at here?
DrAK: Yeah, it’s millimeters. I will say for the face, those are the dermarollers that I’ve seen. And again, I haven’t done extensive studies because I just buy my physician-grade products. But I’ve seen 0.3 millimeters, 0.4 millimeters. You can certainly do those at home and there’s a little discomfort with it in the face, but it’s not anything that you can’t do without numbing cream. Once you get up to one millimeter or one and a half, above that you tend to need numbing cream, unless you’re just a pretty strong and stoic human being.
DrMR: Gotcha. Well, the doctor in my office who does my PRP injection says I have a really fat head, so maybe that will bode well for me.
DrAK: If you have a fat head it actually would be better. It’s the areas of really thin skin like the forehead and the scalp, where you don’t have a lot of fat. That’s when the dermarolling and micro-needling are really painful. So, fat head, there you go.
DrMR: So, the studies use the 1.5 millimeter, but you’re saying for face, 0.3 to 0.4. And what are you thinking for hair? I’ve seen some people recommend 0.5 to one. Would you modify that?
DrAK: Yeah, I would say 0.5 to one is probably good. Once you get up to one … again, it depends on the patient’s face and the patient’s scalp. But once you get up to one and a half or above, oftentimes, A, it’s painful and B, you can oftentimes get some pinpoint bleeding with it. Which is fine if you’re doing it in the right way and you’re a medical provider. But I wouldn’t probably encourage patients to start inducing bleeding on themselves at home, because there’s infection risk and scarring risk and things like that. You want to know what you’re doing before you go really deep.
DrMR: Okay. And with the hair, I’ve read different things. Like you should not use minoxidil/Rogaine after you micro-needle, because the minoxidil may prolong the collagen formation. So is there a simple pre- and post-? Would you say shower and shampoo before and then do micro-needling post? Or would you do the micro-needling first and then shower and shampoo after?

DrAK: I don’t think we really know. We only have a couple of small studies. I believe in both of the ones I’ve seen, they did the micro-needling or the dermarolling, and then they waited 24 hours to apply the minoxidil the next time. Any time you’re doing any micro-needling or dermarolling, you want to make sure you’re not putting something on the skin that is potentially unsterile, irritating, and things like that. So I think that waiting at least a little while is probably a good idea. But I haven’t seen it compared to not waiting, so I don’t know for sure.
DrMR: Okay. Then would you recommend showering after or waiting to shower for a while?
DrAK: You can shower after. I would say, just make sure you don’t have an irritating shampoo. If you had any harsh chemicals or things in your shampoo—which I wouldn’t recommend in general, anyway—don’t put that on your head, but water is fine. That shouldn’t be a problem.
DrMR: Gotcha. And for frequency, do you like the once a week for a month and then every other week thereafter or…?
DrAK: I think once a week is great. Especially if you’re not doing quite as deep as the studies went, then you may just stick with once a week. With hair, it’s often a long-term game. It’s never something that you do one time and you’re done. It’s an upkeep. So whether you’re doing minoxidil, finasteride, micro-needling, I would say get on a regimen and just continue on it as long as you want to keep your hair.
DrMR: Gotcha. And I have to say, when I looked at the follow-up photos from this one study, it’s clear. Now, this is only three cases. But in some studies you can tell the lighting is different, they’ve got product in their hair, making it slicker, so it looks thinner and then the next photo they have nothing in their hair and it’s fluffed up. There was none of that BS smoke and mirrors. It’s pretty significant. For someone looking at their options, I think, maybe it’s a little bit painful while you’re doing the rolling, but it seems like a pretty easy intervention to lead to some benefit (at least based upon what the preliminary evidence says).
DrAK: Yeah. And it’s inexpensive too. It’s accessible to people who are poor. Minoxidil is a generic, you can get it at Costco. So I agree. I think it’s a good first step for people to try for their hair. But keep in mind that the hair cycle is very long, so it may be three months or six months before you see anything. So you have to be patient, you can’t just give it two weeks. It’d seem like, “Uh, this doesn’t work.”
DrMR: Yeah. I believe their first follow-up photos were at two months and then I think it was three and six. At least two to three months with the first. And you did see something at the second and third. But it was really by the sixth month, if I’m remembering the intervals of the photos correctly, where you really saw the big impact.
DrAK: Yeah, that makes sense.
Sponsored Resources
DrMR: Hey everyone. I’d like to thank two companies that can help you to improve your health and have also allowed this podcast to be possible.
Firstly, GAINSWave. GAINSWave therapy can help enhance sexual function by using sound waves similar to ultrasound to both stimulate angiogenesis, or the growth of new blood vessels, and breakdown plaques in existing blood vessels. And GAINSWave has been shown to improve erectile function in men according to two meta-analyses and there have also been 40 clinical trials showing various degrees of favorability in using GAINSWave therapy.

I personally have done one round with Dr. Judson Brandeis, who’s been on the podcast, and I had been very happy with the results of GAINSWave. So if you’re a man suffering, I would not go any longer suffering and I would definitely give GAINSWave a look. They have an offer of one free GAINSWave therapy session if you visit gainswave.com/patient. And for medical professionals, if you want to learn more, you can go to joingainswave.com/provider.
Also, Platinum LED, who makes perhaps the best red light therapy unit on the market. And red light therapy can improve your health by stimulating mitochondria, which make energy for your cells. Now, the research while preliminary has shown encouraging results for an array of applications with red light therapy, thyroid, skin health, anti-aging, joint pain and body composition to name a few.

And I’ve also been using a Platinum LED unit at home and so far I’m really liking it. I do feel like my skin looks much healthier, as has been documented in some of the studies can reduce wrinkles.
Now, in a direct side by side test Platinum LED lights have produced the highest radiants of any led light on the market today. And I’ll link to a cool video for this in the transcript. And this is the coolest part. All their lights come with a 60 day trial period and a full three-year warranty. They’re offering $50 off certain products at platinumtherapylights.com, if you use a coupon code Ruscio50 at checkout. Check them out.
Dermarolling for Skin
DrMR: So what about for the face? Would you also do this once per week? And is there anything that you would modify to be careful? I’m assuming you have to be careful with around the eyes, but any important strokes there for people?
DrAK: Yeah, I haven’t seen as much. There are a number of studies with the face with micro-needling. The difference between micro-needling and dermarolling—just so you know—is dermarolling is like a rolling-pin device. It has needles all around the different sides and you roll it around on your skin. That’s what’s usually sold over the counter. Micro-needling is the same concept. It’s an electrical device. Doctors and med-spas have it. They have needles, maybe 10, and they just go up and down really quickly.
DrMR: I see.

DrAK: Dermaroller needles go in at different angles than they can with the micro-needling, which goes in pretty perpendicular to the skin. And with a lot of these things, you can use either one of them. There are a number of studies looking at micro-needling for skin health, for increasing collagen production, elastin production, and things like that. Again, most of the depths varied from 0.5 millimeters up to about 1.5 or 2 millimeters for skin. But I would say that at home, you don’t want to draw blood. So again, maybe 0.5 millimeters is a good depth for skin. If you could do it once a week, I don’t think there’s any problem with it as long as you’re not causing too much irritation, as long as it’s a light pink. You get light pink and then you’re good after a few minutes.
DrMR: And, is there a concern with the eye area? I’m assuming you can’t do the eyelid. But can you do around fairly proximal around the under eye there, or do you have to be extra-cautious in that area?
DrAK: The skin there is thin obviously. But I just did my own PRP micro-needling like 10 minutes ago, before this podcast. I had a 2.5 millimeter micro-needling device, and I went all the way up to the orbital rim with that. Then I went a little closer to the actual eyeball at 1.5. Certainly at home, you can’t go that deep. I think that as long as you’re careful— the skin around the eye is thinner—0.5, 0.4, or 0.3 millimeters is also not very deep. So you can probably go pretty close to the eye, as long as you’re really careful.
DrMR: Okay. For some therapies like dermarolling, there seems to be some decent evidence—using the hair example—that you can show a notable improvement. I try to be open-minded where this is less “natural medicine,” you could say.
I don’t know if you’ve looked into this or not, but I think some people in our audience would prefer hearing a whole narrative about how a collagen supplement could do the same things. And I’m open to that. But I would guess that if you have a good diet, you may not see a huge improvement beyond what you already have seen, especially if you’re having bone broth and things like that, because you’re getting collagen.
So I try to look for things that are going to deliver bang for their buck. Again, I could be wrong. I know that there are some studies showing that supplemental collagen can have a positive impact, but this would be another way of facilitating results. I guess you could also argue that these may even work synergistically. Do you have any thoughts, Amy, on how the supplement piece factors in and comparative factors in terms of effectiveness?
DrAK: I don’t have any specific thoughts on that part. Collagen, anecdotally, has some evidence that it can be helpful when you take it as a supplement for skin and hair.
The things that I do, like micro-needling and the PRP, I still consider to be very natural treatments. I’m not putting anything into the person’s body or applying anything onto the body that’s not from their body. I have a lot of patients that come to see me who don’t want to take medications. They don’t use any chemicals, they don’t use sunscreen, they don’t use anything. But they feel, as I do, that we can use technology, like micro-needling, to help their bodies heal themselves. That’s pretty natural, I think.
DrMR: Absolutely agreed.
Minoxidil for Hair Loss
Regarding Rogaine, I think some people in our audience may be a little bit less comfortable with it. I haven’t looked into the side effect profile. I do know, of course, there is some evidence showing favorability using Rogaine. I also know that it’s recommended to use it twice a day, but I think that might be hard for people.
As someone who’s tinkered with Rogaine, it seems like doing it before bed is pretty easy. Doing it first thing in the morning, the stuff stays in and sometimes it makes your hair look a little weird.
With Propecia (finasteride), which we’ll come to a bit later, there’s a five milligram. There’s also a one milligram. As far I have been able to tell, the one milligram pretty much gets you the same results as the five milligrams. I’m not sure with Rogaine if using it once a day gets you a pretty close benefit to twice a day. I’m wondering what you think about that. And then what are your thoughts on any side effects with Rogaine?
DrAK: I haven’t looked into whether using it once a day is as effective as twice a day. I know that twice a day is what’s recommended. There are different formulations. Rogaine is the same as minoxidil, the 5% is what’s most commonly used for men and even for women. I recommend 5% usually. But most people don’t have any problems with it. It doesn’t usually cause irritation.
It can be a little annoying. Some people, like you said, don’t want to put it on before they go to work because it makes their hair look sticky. But there are other formulations that you can get. Some of them can be compounded or specially ordered: liquid, gel, foam. There are all different ways to apply it. I think not everyone likes minoxidil, but it does work. If you’re consistent with it, it works pretty well, or at least better than most other things that we sometimes think work.
Philosophy of Hair Loss Treatment
DrMR: Okay. I’ve previously talked about lasers. This might be actually a good point in the conversation to clarify what I think your overarching philosophy is with hair. And again, correct me if I’m wrong, but I think it’s pretty smart. That is: throw everything you can at improving your hair health, and get to the objective that you’re looking to get to, which is preventing loss, looking thicker, looking healthier. Then maybe you can consider trying to wean down and finding the minimal effective protocol.
But I think what happens with people is—and again I could be wrong, but I’m just thinking about conversations I’ve had with friends and with patients—they try one therapy, they do it for a few months, they don’t see huge change and they abandon it. Then they do another one. And they go through this merry-go-round for a couple of years, all the while seeing a regression in their hair health. Only then do they finally say, “Okay, I’m just going to do everything,” and that’s when they finally start to see some results.
If we could get people to understand this should be more of a top-down approach, as it’s known in conventional medicine– meaning, give all the therapies and then consider weaning down—that might be a better way to approach this. Is that a fair encapsulation of your philosophy?
DrAK: That is my philosophy. I agree with you. Hair loss is really difficult, and right now we just don’t have the magic pill that’s going to fix everything and for everyone. I see so many people who will come in and get one PRP treatment. Then it doesn’t work and they’re like, “Oh, that didn’t work.”
Or they’ll do minoxidil for a month and then they stop, just like you said. First of all, if you don’t care about your hair loss, then that’s fine. You don’t have to do anything. But if it bothers you and you want to maintain your hair, I think doing as many of the things as you’re comfortable doing is going to be the most effective way to keep your hair.
Low-Level Light Therapy for Hair Loss
DrMR: And we’ve talked about a few of these. Let’s talk briefly about laser. I think lasers have a lot of cool applications and there have been a number of studies showing benefit with laser. I believe there’s at least one comparative trial looking at the comparison to minoxidil/Rogaine showing similar results.
Again, will lasers work for everyone? No. Will it take at least three months, maybe closer to six to see any results? Probably. But it’s one of these numerous things, including collagen, oral DHT blockers whether saw palmetto or finasteride, dermarolling, and then Rogaine, you can use to hit this from multiple angles so as to have the best outcome. There does seem to be evidence to support this. But what’s your experience with lasers? Do you have any devices that you really like?

DrAK: Yeah. So laser therapy for hair loss is low-level light therapy or red light therapy. And there are a number of devices now that have come out. Capillus was one of the first ones, early to the game. There are other ones now, like iRestore. These caps have red light or low-level light therapy that comes out of them. You just put it on your head and it’s like a baseball cap. You can wear it around and you’re in for 20 or 30 minutes, a few times a week. We know from other low-level light therapy studies on skin, and other things, that they work by activating ATP production in the mitochondria. The same thing happens with hair.
So, it’s definitely a great adjunctive treatment, meaning you can add it to other treatments. You’re totally right: it takes a good six months to see results, but it’s also completely safe. There’s no side effects. There’s no downtime, there’s no pain. And aside from the cost of the hat or the laser, it’s really easy. You could do it at home, while you’re watching Netflix. So I do like the laser therapy and I recommend that as something for my patients to do when they go back home.
DrMR: Looking at the devices, the two that I liked the best are either the Hairmax laser comb or the iRestore laser cap. The laser cap is good if your hair loss is predominantly on the top of your head. But if you have a lot of thinning and loss on the sides, it doesn’t look like the laser cap really gets the side. If you’re wearing a hat, it doesn’t really get in front of your ears.
So that’s where the laser comb comes in: you can really comb wherever the area is, and get the laser in that area. Whether or not that has a clinically-discernible benefit, one versus the other, that hasn’t been determined. But it just makes sense that if the cap sits on top of your head and that’s the region where you have your loss, that would work well for you. And if your hair loss is not consolidated at the top and you have some on the sides, using a device where you can get in that area may lead to better results.
DrAK: Yeah, I think you’re right. You definitely want to put it where the hair loss is. But you have to keep in mind that want to have it on there, generally depending on the laser, for 20 minutes or more per session. So the ones that you could just put on your head are easier in that regard.
Certainly doctors’ offices, ones who deal with hair loss, will have a lot of the even stronger lasers that you don’t have to do quite as often. They’re really strong. But generally, looking at red light therapy with wavelengths in the 630 to 670 nanometers or so for this, there are a lot of different devices out there that can be effective. I would say wherever your hair loss is, just make sure that you’re covering that spot.

DrMR: So question there. And pardon me if this is getting too into the details and if you haven’t gone this deep into some of these particulars, but the application of the Hairmax device and the iRestore seem to be pretty different. For the Hairmax device, you stay for a couple of seconds, in this one small band where you have a laser beam. Then you move. So it’s two seconds per region, then you comb forward, then it’s two seconds and comb forward, two seconds, and you do the whole head in about eight minutes.
Whereas the iRestore, I believe, is not so much using laser but more using a diffuse LED. And you’re getting the whole area, but you have to keep it on that area for about 20 minutes. It does seem that both devices have literature to back them up, but if one of those is better than the other, I’d be very curious to hear your thoughts on that.
DrAK: I haven’t seen a comparison between the different types of hats, helmets, combs and things. Certainly, part of how long you have to keep it on a given area depends on how strong the laser is, how much laser light it’s putting out. But aside from that, I don’t know really what the best ones are out there. I know some of the ones that have been out there the longest. There are so many new ones that are coming out all the time that I think that there’s probably utility in all the major brands. But I haven’t done a comparison myself.
PRP Injections for Hair Loss and Skin Health
DrMR: Okay. And let’s talk about PRP. We had a guest on who talked about hair injections for PRP, but maybe give your short primer on how you like to use it for hair, the kind of effects that you see. And then share how you like to use it for skin and the effects you see there.
DrAK: So PRP is just made from centrifuging a patient’s own blood and getting the platelets. We’re looking for a platelet concentration, usually about seven to nine times that of whole blood. So we want to get about a million platelets, versus 250 per area.
For hair, there are a number of studies that do show utility of using PRP for hair, overall, if you average them together. If you do three treatments of PRP injections in hair and you do them about a month apart, then generally you’ll have between 18 and 33 new hairs per centimeter. This is mostly for male androgenic alopecia. That 18 to 33 new hairs is a decent amount per centimeter squared, and then apply that to the whole head.

Most of these studies are split-head study. So they’re doing the protocol with the PRP on one side of the person’s head and then they’re doing normal saline or some other placebo on the other side, which is a great way to do it because it’s the same person. You’re able to really compare apples to apples there. All of the studies that I’ve seen with PRP that were effective do at least three treatments of PRP.
There was one study that came out in the last year or so, where they just did one treatment of PRP and were seeing if that was effective. In that case they said no, it wasn’t. So there seems to be something about doing several of them that’s important for it to actually work. Then there are other studies that have compared PRP plus Minoxidil to PRP plus finasteride. Like, which one of those is better?
There are all different sort of iterations of using these combinations for patients. People understand that you’ve got to use several things most of the time. I find that in practice, the PRP can be great. It can definitely cause improvements in hair. But there are some patients, with all PRP procedures, whether it’s hair or joint or skin or anything, that just don’t respond as well as I would like them to. And I don’t know why. I don’t know if it’s the health of the patient, the health of the platelets, if it has to do with lifestyle or other things. I find it really frustrating, because obviously I want it to work for everyone, and it doesn’t always. But it does work for the majority of people, and I think it’s a great natural way to treat hair loss.
DrMR: What would you say is the protocol: give it this many months doing a treatment once a month? And then if you haven’t seen a result by x point in time, it’s time to look at something else?
DrAK: All the studies that I’ve seen that have worked, again, have been three treatments at four to six weeks apart. The tough thing about that is, you’re doing all three treatments, essentially, before you even know if they’re going to work. It takes three to six months before you can see results. So it could be a little frustrating because patients don’t want to do multiple treatments. That can be uncomfortable, sometimes expensive, if they’re not going to work, but that is what’s been studied as far as getting results. So I do recommend that.
I just recommend do all three, at a space of about a month apart. If you’ve had three and you’ve also addressed all the other things that can cause hair loss and you’re still not having results, then certainly you can do more, but it may not be beneficial if it didn’t work the first time.
DrMR: I’m assuming that people are looking for both the thickness and the fullness of their hair, but also, is a degree of falling hair something that people are also using as a way of monitoring this?
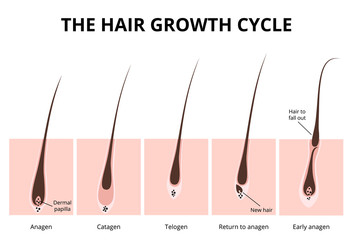
DrAK: Yeah. Sometimes in the beginning, right after these kinds of treatments, like the PRP treatments for example, some people actually have increased hair loss for a period of time, which can be disconcerting, as you might imagine. But if you think about what we’re trying to do, it actually makes sense.
What we know about hair loss in general is that patients spend more time in what’s called the telogen phase. So their hair is spending more time in this almost-going-to-fall-out stage or the pre-death phase. Whereas in a person with a healthy head of hair spends two to seven years in the anagen phase, or the growth phase. So what we’re trying to do with PRP is shift a hair cycle from the telogen phase to the anagen phase. Oftentimes, the hairs that are already in the telogen phase—telogen hairs are often called miniaturized hair, and are thin, small and sparse—will fall out first, before the hair cycle can get back to the anagen phase and give you better, stronger hair.
So having some hair loss right after you get a PRP procedure, even starting minoxidil or things like that, isn’t necessarily a bad thing. It oftentimes is a good thing because you’re restarting that hair cycle.
DrMR: Yeah. I do think that’s worth stating. And I know that some of the laser literature purports the same thing: you may see increased shedding or increased falling hair for the first couple months before you see improvement. So I think that’s really important for the consumer to be aware of so that you don’t jump ship prematurely.
DrAK: Absolutely. It makes people obviously very nervous when their hair starts falling out even more and they’re just like, “What did you do to me?” It’s important to know that’s normal.
Finasteride for Hair Loss, Side Effects
DrMR: I want to touch on exosomes and stem cells, but I’d like to come to Propecia, or finasteride, next. There was a long while where I was quite against the prospect of using Propecia or finasteride because of the purported sexual side effects. There’s even one study that looks at Postfinasteride syndrome(PFS), where men were having these sexual side effects that were purported to persist even after stopping the finasteride. That to me just seemed like a huge red flag.
But recently I’ve been checking this. I know that, like many things I’ve fact-checked, the narrative and the actual evidence are quite different. You and I have spoken on this recently, but there was recently a meta-analysis published showing that when you look at these studies, factor in for placebo, and do a good job of studying this, the incidence of sexual side effects in men taking finasteride is only about 2-3%. So it’s fairly insignificant.
And I’ve also been talking with Dr. Turek, who we’ll be having on the podcast at some point. He’s writing a chapter about finasteride in a textbook for publication in the future. And he’s been looking into this data more closely. He’s finding that for many of the people who tend to have those reported side effects, this post-finasteride effect, are actually suffering from other comorbidities. They may have depression, porn addictions, or gender identity issues. He’s finding that that subset of the population is quite densely concentrated into those who are reporting this Post-finasteride Syndrome.
We look at that, combined with the fact that as men age, the percentage of erectile dysfunction goes up as you go from your 20s to 30s to 40s to 50s. I think by the time you get to your 50s, it’s 40%—maybe even 50%—of men report some type of sexual dysfunction. So as you get older, there’s a higher chance that you’re going to go on Propecia. And as you get older there’s a higher chance you’re going to have erectile complaints. It would make sense that age may be a confounding variable here that is being left out of the equation, and people are just saying, “Well, it must have been the finasteride that I took.”
I just think it’s important to be objective. When I have discussions about hair loss with men in my clinic, some of them get quite emotional and quite distraught about this, and understandably so. It’s something that for some men is a very emotional issue. So we should be careful not to be irresponsible in how we’re citing data regarding finasteride or Propecia. Because if the side effects are minimal, and if they’re being way over-reported, that’s thwarting someone from potentially using a medication that could help them. So I think it’s worth at least having a second look. I don’t profess to know all of the nuances of the side effects of finasteride, but the sexual dysfunction one is one I’ve looked into. And it does look like the side effects are actually over-reported, and fortunately it’s only about 2-3% of subjects.
DrAK: Yes, that’s exactly right. I have a lot of patients obviously who will come in and they have been on finasteride in the past. They aren’t even on it anymore and they’ve been off of it for years, they start having erectile dysfunction, and they’ll blame the finasteride, saying, “What can I do about this finasteride-induced ED?” But again, they’re 45, they’re 50, they’re overweight, they have other problems sometimes. So I totally agree that the actual rate seems to be really low with finasteride. And dutasteride, a newer one, which is another dihydrotestosterone blocker. It seems to have even lower sexual side effects.
So I think those are two options. Certainly it’s up to every patient to decide if they want to take a medication for that. You’re blocking the conversion of testosterone to DHT, and in males who have male pattern baldness, it’s the DHT (the dihydrotestosterone sensitivity at the hair follicle) that is oftentimes responsible for a lot of the hair loss. So if you can decrease the amount of DHT you have, it can make a big difference.
DrMR: Now, is the reason why some men have hair loss and others don’t the density of DHT receptors in the scalp between different men? Is that what dictates this?
DrAK: I don’t know exactly. I do know that it’s not necessarily about the DHT level. Certainly if you have very little DHT, then you’re going to have less of a problem with hair loss oftentimes. But at the same time, I think when you have normal or high DHT, sometimes you don’t see any difference in hair loss and sometimes you do. So it seems to be that some men are just much more sensitive to the DHT. But I don’t know if it’s number of receptors, how well they work, signaling, or what other things are responsible.
DrMR: Gotcha. So it’s some genetic variant, said loosely.
DrAK: Yeah.
View Dr. Ruscio’s Additional Resources
DrMR: Let me check in on one other thing. When we were fact-checking some of this stuff regarding Propecia/finasteride, we also looked at the dose effect. Arguably if you can be on the lowest effective dose, then you would mitigate the chance for any kind of side effect, even though the side effects do seem to be fairly small. And it does look like one milligram of finasteride (I didn’t look deeply at dutasteride) was about as effective as five milligrams. So it seems you can get away with quite a lower dose of one milligram than the five milligrams, and have the same effect on the hair.
DrAK: Yeah. So Propecia is essentially one milligram finasteride. Finasteride is the generic form of the medication. It’s a lot less expensive usually for patients, if you give them a five milligram tab. I just have them cut it in quarters and take one quarter a day. That ends up being quite a bit less expensive generally than getting Propecia, which is a labeled medication. They charge a lot more for it because it’s just for hair loss. But you can just take regular finasteride, it works just as well.
I believe that there was a dutasteride study that did show that the higher level of dutasteride versus the lower level helped a little bit more. But you also have to weigh things, like how much is this medication going to cost? And is that benefit going to be worth it or not? Most of the time I think it’s probably not worth it to take the higher dose of these things.
DrMR: The dutasteride has a lower incidence of side effects?

DrAK: Yeah, I believe it has a lower incidence, although neither one has a lot of side effects. Dutasteride is a lot newer.
DrMR: I was just going to say, could it be the newness effect?
DrAK: It could be. It could be that people don’t know that they’re supposed to have side effects from it.
DrMR: And this has also worked for women.
DrAK: It can. A couple of things you have to know about it. First of all, it can work for women if they have the male pattern baldness, the androgenetic alopecia, which again is the most common reason for women to have that. But you wouldn’t want to put a woman on finasteride, in general, if that’s not the reason for their hair loss. There are some genetic tests that can be done, that could look to see if that’s the reason for their hair loss. And if so, then you can do finasteride for women, just like you can for men.
DrMR: What’s the test?
DrAK: Oh, I knew you were going to ask that. The one that I used to use, they stopped doing it. So now I don’t know what the best one is for it now.
DrMR: Gotcha. Fair enough. And because we’re talking about a bunch of different therapies here, is this a therapy you would say is one of the most effective? I know it’s fairly popular. Is it popular by reason?
DrAK: Yes. Finasteride really helps decrease hair loss with androgenetic alopecia as well as helps you to gain some hair as well. But again, you’ve got to combine it with the other things as well, if you really want to see the best results.
DrMR: Gotcha. Okay, good to know.
Stem Cell Therapy for Hair Loss & Skin
So final couple therapies here are exosomes and stem cells, which are kind of similar. I’m still a little fuzzy on what the difference is exactly. Can you get us up to speed on these: what they are, how you use them, and anything else?
DrAK: Yeah. So stem cells are the cells that are in every different tissue in your body. They’re responsible for keeping that tissue up. Whether you get injured or sick or the cells die, the stem cells are the ones that can replicate and differentiate. They can become all different tissues in the body. So they’re very important in that regard.
There are some therapies now for both hair and skin, where we can take stem cells from the patient. You can get it from the fat, you can get it from their bone marrow. You can get other stem cells from other people. Essentially you can take stem cells from one part of the patient’s body and put them somewhere else. You could put them into the skin of the face, inject them in the hair, or put them in the joints.
And what that essentially does is it communicates with the patient’s own stem cells that were already in that part of the body. It tells them, “Hey, stop being so lazy. Let’s get back to work. Let’s start making more hair, let’s start making more collagen, let’s start making more hyaluronic acid and elastin and all the things that we stopped producing as much of as we get older.” So stem cell therapies—as well as exosomes, which are like little messengers—are ways that we can jumpstart the patient’s own stem cells. They’re communication tools to jumpstart your own stem cells’ regenerative capacities, no matter where you put them.
DrMR: You’re doing this escalation, where if someone’s really motivated, they start with PRP. If PRP doesn’t work, then you graduate to exosomes. Then you finally graduate to stem cells. Is that the way that you’re flowing this?
DrAK: It depends on the patient. The exosomes are a product that we can buy. They’re made from umbilical cord stem cells in a lab, and they get frozen. Essentially, these exosomes are like the messengers from the stem cells. So these umbilical cord stem cells will release exosomes, which contain a bunch of information, into the lab culture. We can take it and just filter out the exosomes. So the exosomes are kind of like doing a stem cell therapy, but you’re not giving the patient genetic information from someone else. All you’re giving them is the growth factors part of it.
And again, with hair and with skin, there’s not a ton of information out there yet. There aren’t a ton of data. Definitely animal studies. There are some human studies, but they’re small, looking at stem cells and exosomes in skin and hair. So we’re very early in looking at that. But yes, I will use exosomes, in addition to PRP, for hair and for skin.
Then in some patients, I’ll use stem cells, but usually only if they’re already getting their stem cells taken for something else. Like because they’re going to get stem cells taken to be put in their joints. Then I’ll use some and put it in their skin and their hair as well. But because it involves a procedure to do that, and because the data are not great yet, I think it’s best not to have to put them through that, if we don’t know exactly how much better it is than just PRP by itself.
DrMR: And are you finding that the exosomes give you a noticeable increase in efficacy?
DrAK: I do think—this is all anecdotal, meaning that I don’t have research to back it up, it’s just my patient population—that the combination of PRP plus exosomes is more effective than even the PRP and stem cells, in the hair patients that I’ve seen. And also maybe the skin. The exosomes are really tiny, much smaller than stem cells. And maybe that’s why, but they can really penetrate deeper into the skin. That may contribute to why they’re so effective, only because they’re coming from umbilical cord cells which are new, very healthy, very youthful cells versus the patients themselves (who are obviously not quite as youthful).
DrMR: With the PRP, plus or minus the exosomes, it seems that you do a treatment every month, usually for three months until you see results. And then from there, do you agree with the recommendation that you do one treatment every three months thereafter?
DrAK: If you can. Most people don’t have the ability to do it that often. Most of the patients that I see will do three treatments once a month for three months. Then they’ll come back in maybe a year, because most of PRP lasts a year to a year and a half. And they’ll maybe get one or two or three more treatments, depending on how effective it was the first time and how they’re doing.
PRP Versus Micro-Needling for Skin
DrMR: Gotcha. Okay. And then, we didn’t touch on PRP for skin. If you were to compare that with dermarolling, would you say they’re equally as effective? PRP is obviously a bit more expensive, a bit more invasive. Is it worth that additional cost and trouble?
DrAK: So there are studies that look at micro-needling (again, similar to dermarolling) and applying water afterwards only, versus micro-needling with vitamin C, versus micro-needling with PRP. First of all, what they noticed was that all of them showed benefit, with even just water. Micro-needling alone does show benefit in terms of skin health and collagen production and such. But definitely the micro-needling with PRP was better than the other two. So you got better improvement in fine lines, texture tones, and things like that.

A lot of times because PRP is a little more expensive, I will have patients do the micro-needling with PRP on the first treatment. And then the second and third treatment we might just do micro-needling with hyaluronic acid, vitamin C, or some other growth factors that can be much less expensive and not require a blood draw. We’ll do it like that sometimes in patients if they don’t want to or can’t afford to do PRP every time.
DrMR: So someone could likely—if they were trying to do something at home—do dermarolling with, let’s say a 0.3, 0.4 or 0.5 millimeter dermaroller. Is there a vitamin C cream or hyaluronic acid cream to combine that with? A certain cream over the counter that people could use in that application?
DrAK: If they’re just doing a 0.3 or something like that, yeah. There are a bunch of different hyaluronic acid and vitamin C creams. You can use any of them, really, as long as you’re not going too deep. If you’re going really deep, you’d want to have a sterile serum that was made specifically for micro-needling. You don’t want to be applying anything that’s not sterile into the dermis, the deeper layer to the skin. So I think that home dermarolling can certainly be helpful, but it’s not the same as it is coming into a doctor or med-spa and getting a deeper treatment. We’re able to go so much deeper and you’re going to get much better results with that deeper treatment in a medical facility than you are at home. But you can do both.
DrMR: Gotcha. Cool. Well, that’s a litany of options for people. We hit on a lot of different therapies for skin and hair. And hopefully for the audience this helps maybe dispel some myths, mainly around finasteride. Also, if nothing else, it gives you a perspective on the available therapies. If it’s something, especially hair, that’s really important to you, come at it aggressively and figure out what works. Then from there you can try to pare down and find the minimum effective dose or assortment of treatments. I’ll be curious to hear the audience feedback on this.
Episode Wrap-Up
And Amy, as we transition to a close, do you have any parting thoughts? Then please tell people your website, blog, anywhere that you want to point them on the internet to connect with you.
DrAK: Yeah. First of all, thank you so much for having me. This was really fun, I love diving into the nitty gritty questions with you. I don’t always have the answers, but I love it. I have several different websites. The easiest way to find me is just DrAmyKillen.com, and that website will point you to the other websites. I have several different clinics that I operate out of and do all different things. And then on social media, I’m @Dr.AmyBKillen on Instagram, Facebook, all of that. I try to keep those things up to date as well.
DrMR: Sweet. It was a lot of fun. Thank you for taking the time. And if there’s anything really interesting that crosses your desk, please let me know, and maybe we’ll have you back on and expand upon something.
DrAK: Sounds good. Thanks a lot. Have a good day.
DrMR: Thank you.
Dr. Michael Ruscio is a DC, natural health provider, researcher, and clinician. He serves as an Adjunct Professor at the University of Bridgeport and has published numerous papers in scientific journals as well as the book Healthy Gut, Healthy You. He also founded the Ruscio Institute of Functional Health, where he helps patients with a wide range of GI conditions and serves as the Head of Research.➕ Resources & Links
- Simple Keys for Ending Your Joint Pain Using Regenerative Injection Therapies with Dr. Tyna Moore
- Postfinasteride Syndrome (PFS): Investigation of the Plausibility of 5-Alpha-Reductase Inhibitor Syndrome
- Adverse Event Reporting in Clinical Trials of Finasteride for Androgenic Alopecia: A Meta-analysis
- Irestore laser cap
- Laser comb
- dramykillen.com
- Dr. Amy Killen on Instagram and Facebook
- Gainswave.com
- JoinGainswave.com
- Platinumtherapylights.com
- Dr. Ruscio Resources
Discussion
I care about answering your questions and sharing my knowledge with you. Leave a comment or connect with me on social media asking any health question you may have and I just might incorporate it into our next listener questions podcast episode just for you!