Practitioner Case Study – February 2017
Dr. Michael Ruscio’s Monthly – Future of Functional Medicine Review Clinical Newsletter
Practical Solutions for Practitioners
In Today’s Issue
Case study
Research
- Low carbohydrate diets improve thyroid autoimmunity.
- Insufficient documentation for clinical efficacy of selenium supplementation in chronic autoimmune thyroiditis.
- Berberine successful for IBS, but there is a twist.
- Probiotics in IBS, a review of the literature.
Practitioner Question of the Month
Practice Tip
![]()
Case Study
*Note: this is a long case study but it does teach us a few valuable lessons.
Patient Info:
- June, 63yo, female
- Previous dx: hypothyroid
- Rx: 125 mcg Levothyroxine
- Chief Complaints:
Visit 1 (day 1) – History and Exam:
June had previously responded well to the paleo diet, she; lost some weight, had better energy, noted her joint pain went away and that her stomach aches were gone. She also clearly noted she does not do well with dairy or gluten. Even though dietary changes were helpful she then hit a plateau and was left with the above symptoms. She had a family history of Hashimoto’s, suggesting her hypothyroid was due to autoimmunity.
All lifestyle factors seemed to be in good order. She responded very well to thyroid Rx when she had initially started treatment. She also exhibited many signs of adrenal fatigue and female hormone imbalance (fatigue, caffeine dependence, irritability, insomnia, hot flashes, decreased libido, brain fog, vaginal dryness, depression/anxiety).
Initial impression
- I suspected that June had some gastrointestinal dysbiosis, adrenal fatigue, female hormone imbalances and thyroid autoimmunity as the main underlying factors contributing to her sequelae. The fact that she had noted a strong aversion to gluten suggests she may be NCGS, which may increases the chances of subsequent dysbiosis. It also suggest she may need to adhere to more strict avoidance in the long term.
- I was not overly concerned about thyroid hormone conversion or levels since she noted a very positive response to her initial thyroid Rx.
Visit 2 (a few days later) – Testing and Initial Recommendations
Testing
- Custom blood panel, LabCorp
- – CBC w Diff & platlet count
- – Metabolic Panel, Comprehensive
- – Iron Panel: iron, TIBC, Iron Sat., Ferritin
- – Thyroid-Stimulating Hormone (TSH)
- – Thyroxine, Total (T-4, Total)
- – T3, Total (Triiodothyronine, Total)
- – rT3
- – Homocysteine
- – Thyroid Abs
- Diagnostechs select panel of 15 markers
- Medical Diagnostics Laboratories infection panel
Recommendations
- Diet: autoimmune paleo diet
- Hormonal: Bioidentical HRT cream (estrogen/progestogen mixture), adrenal adaptogenic herbal blend
- GI: Lacto/bifido probiotic, digestive bitters
Visit 3 (day 30) – Lab Interpretation and Treatment Evaluation
Lab interpretation:
-
- Custom blood panel
-
- – Unremarked other than Hashimoto’s

-
- Diagnostechs select panel of 15 markers
- – Main finding is H. Pylori
- Custom blood panel
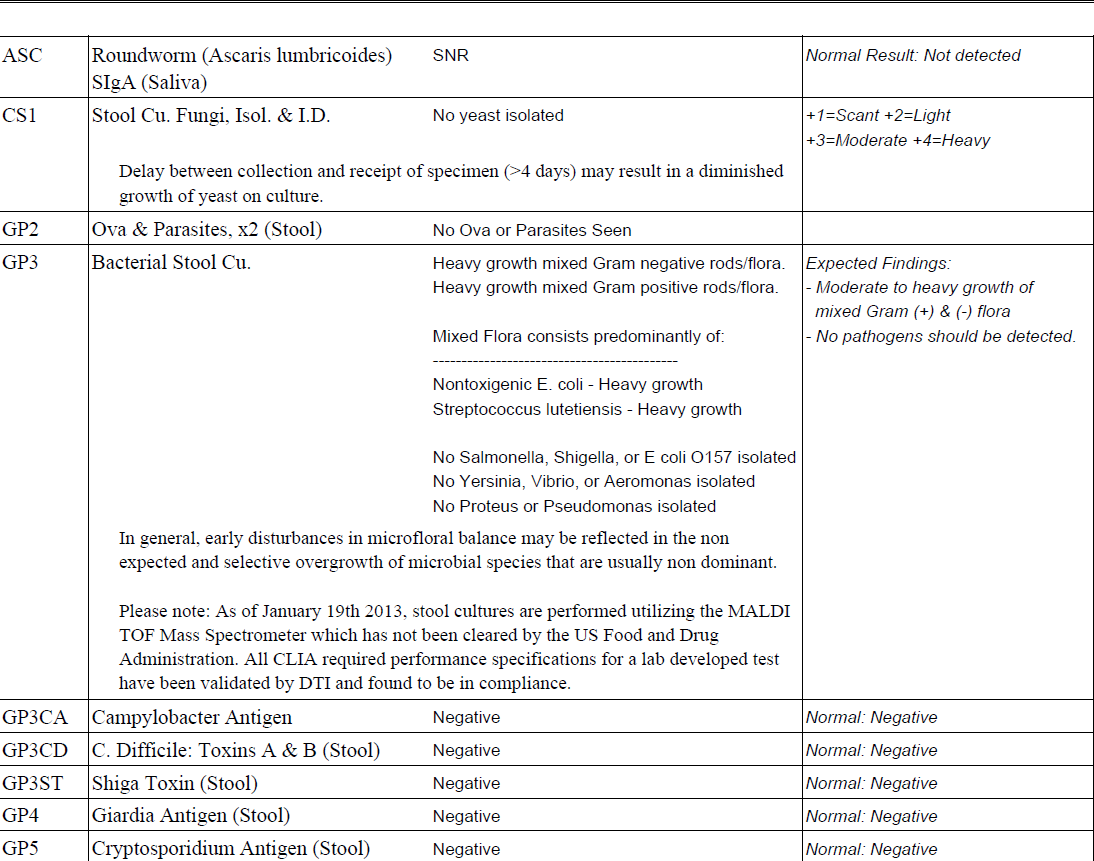
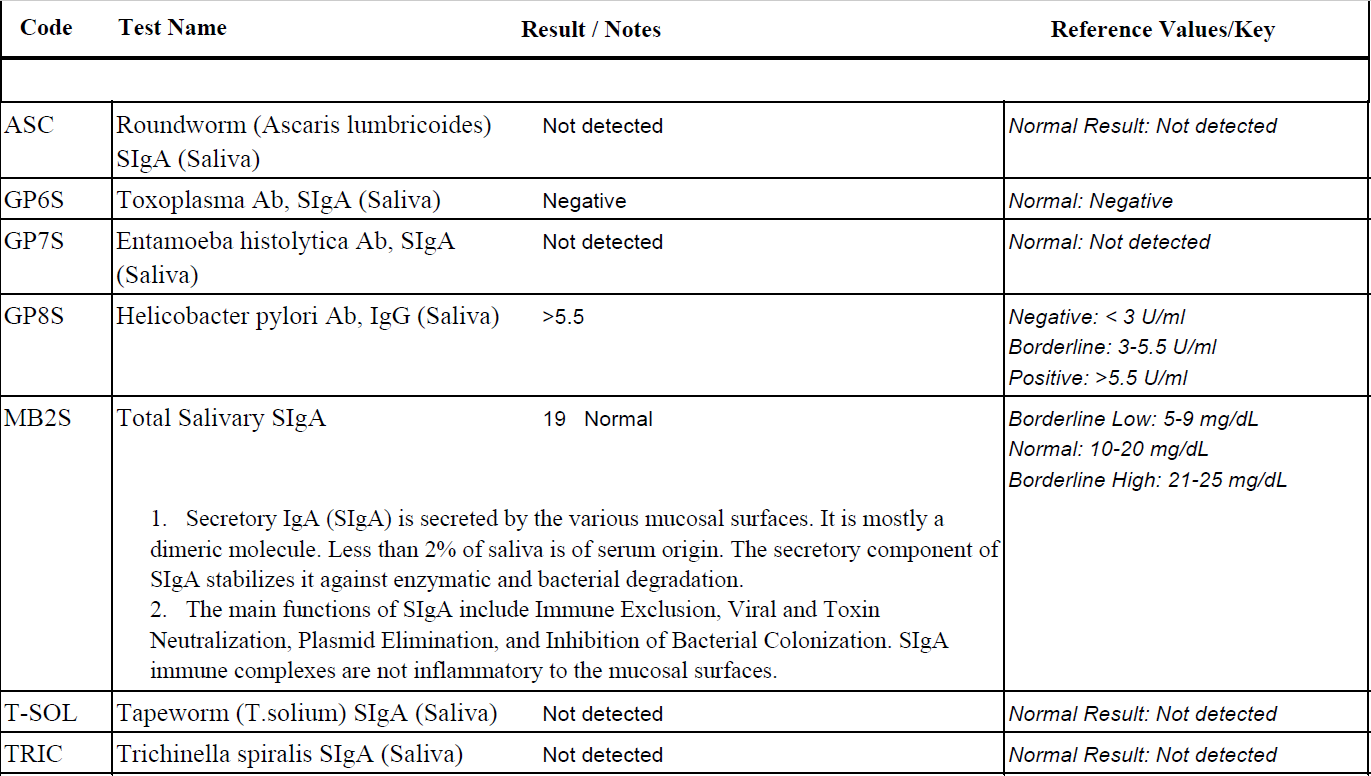
- Medical Diagnostics Laboratories infection panel, main findings (lab image too large to include).
- – H. Pylori IgG and IgA positive
- – EBV reactivation
Subjective Assessment
- Digestion “way better”
- Improved; energy, sleep, cravings
- Weight loss: 4-5lbs
- Can now tolerate eggs
Impression:
- Dietary changes, adrenal support, female hormone support and digestive support are working nicely. Treatment of H. Pylori and/or EBV may lead to further symptomatic improvement and reduction in thyroid abs. We will start with her GI and then consider anti-viral treatment.
Recommendations
- Maintain previous program
- – Diet: autoimmune paleo diet
- – Hormonal: Bioidentical HRT cream (estrogen/progestogen mixture), adrenal adaptogenic herbal blend
- – GI: Lacto/bifido probiotic, digestive bitters
Visit 4 (day 60)
Subjective Assessment:
- Improved
- – Energy, way better
- – Lost 10lbs total to date
- – People are saying she looks great
- Worse:
- – Digestion, since starting herbal Abx – bowel changes, stomach aches
- – Itching, irritability
Impression:
- Overall we are moving in the right direction as evidenced by the aggregate of her symptomatic findings. However, herbal antimicrobials appear to be causing irritation – which I expected to dissipate once the course was through. I did however recommend she take the remainder of her course of antimicrobials with food to mitigate any reaction.
Recommendations:
- Maintain previous program;
- – Diet: autoimmune paleo diet
- – Hormonal: Bioidentical HRT cream (estrogen/progestogen mixture), adrenal adaptogenic herbal blend
- – GI: Lacto/bifido probiotic, digestive bitters
- Continue with antimicrobials but take with food instead of on empty stomach.
Visit 5 (day 90)
*June had just previously finished a 2 month course of herbal antimicrobials.
Subjective Assessment:
- Improved
- – Weight has now gone from 164 lbs. originally to 151 lbs.
- – June has maintained all previous improvements
- – The GI irritation, anxiety and irritability have now subsided
- Worse:
- – N/A
Impression:
- Any reactions previously were from the antimicrobials and are now cleared. Overall June is doing great. We will wait 60 days to allow antibodies to fall and then retest. We will also have her start on her food reintroduction.
Recommendations:
- Maintain previous program;
- – Diet: autoimmune paleo diet
- – Hormonal: Bioidentical HRT cream (estrogen/progestogen mixture), adrenal adaptogenic herbal blend
- – GI: Lacto/bifido probiotic, digestive bitters
- Perform dietary reintroduction to normal paleo diet, avoid any foods that cause a negative reaction
- Wait 60 days and then perform retesting
- – Perform retesting of LabCorp blood panel
- – Retest previous findings from Medical Diagnostic Labs but through LabCorp to utilize insurance
Visit 6 (month 6)
June has now been off antimicrobials for roughly 3 months, and has performed dietary reintroduction.
Lab Findings:
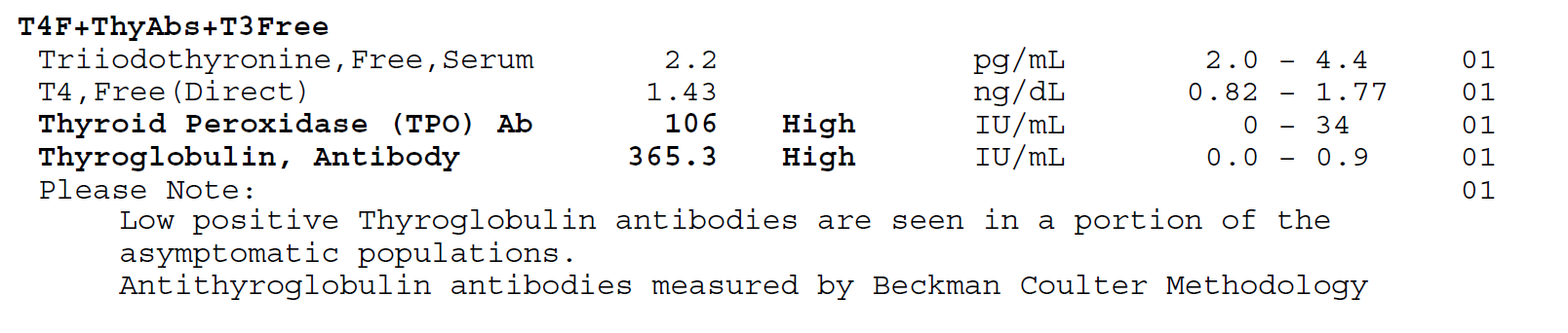
- Retesting of LabCorp blood panel
- – fT4 1.47 to 1.85 (high)
- – TPO 106 to 103
- – TGab 365 to 201
- Retest previous findings from Medical Diagnostic Labs but through LabCorp
- – EBV; EA IgG 671, VCA 199, NA >600 *early antigen, viral capsid antigen, nuclear antigen
- – HP IgG >8, IgA 16.6
Subjective Assessment:
- Improved
- – June has maintained all previous improvements
- Worse
- – N/A
- She has noticed she does not do well with nuts or chocolate
Impression:
- Any reactions previously were from the antimicrobials and are now cleared.
- June needs to generally avoid gluten, nuts and chocolate.
- June may need to decrease her thyroid Rx, likely due to enhanced GI absorption. However, June and I decided for us to focus on her gut and thyroid autoimmunity and have her endo make dose adjustments to thyroid Rx as they aredeemed necessary.
- Thyroid autoimmunity has improved slightly. EBV and HP are still positive – hard to gauge if they have improved because we have retested with different lab. Her marked symptomatic improvement make these results less concerning.
- Overall June is doing great but perhaps we can get her thyroid antibodies lower with additional treatment.
Recommendations:
- Maintain previous program
- – Diet: autoimmune paleo diet/normal paleo diet hybrid based upon reintroduction
- – Hormonal: Bioidentical HRT cream (estrogen/progestogen mixture), adrenal adaptogenic herbal blend
- – GI: Lacto/bifido probiotic, digestive bitters
- Starting a 2-month round of H. Pylori treatment and starting antivirals
- – Curtailed H. Pylori treatment: mastic based formula combined with anti-biofilm cocktail
- – Antivirals including: monolaurin, Reishi, silver, and quercetin
- – Wait 30 days after completing this protocol and then retest (H. Pylori and EBV).
Visit 7 (month 9)
June had recently completed a 2-month round of HP and EBV treatment.
Lab Findings:
- LabCorp retest (H. Pylori and EBV).
- – HP IgG >8, IgA 18.4 *essentially no change*
- – EBV EA 51.1 *previously was 671, major improvement*
- – Note: we retested only the EBV EA (early antigen) as this may be the most important fraction to dictate treatment response.
- Subjective Assessment:
- – June has maintained all previous improvements
- – She had not noticed any additional improvement with this last round of treatment
Impression:
- June is doing great symptomatically and so we will start to curtail her treatment program, we will start with weaning off the bioidentical hormone support.
- Additional treatment of H. Pylori did not provide any additional benefit to her symptoms nor to her labs, suggesting these levels may be normal for her.
- EBV treatment did lower her EA (early antigen) fraction significantly.
- We need to assess if this has impacted thyroid autoimmunity in the near future. We should also retest HP and EBV antibodies one more time to monitor activity.
Recommendations:
- Continue on this program
- – Diet: autoimmune paleo diet/normal paleo diet hybrid based upon reintroduction
- – Hormonal: adrenal adaptogenic herbal blend
- – GI: Lacto/bifido probiotic, digestive bitters
- Slowly wean off bioidentical hormone support
- Wait 1.5 months and then retest H. Pylori and EBV again.
Visit 8 (month 11)
Lab Findings:
- LabCorp retest H. Pylori and EBV).
- – EBV EA 44.6 *essentially no change*
- – HP IgG >8, IgA 23.5 *essentially no change*
Subjective Assessment:
- June has maintained all previous improvements
- Weaned off hormonal support without any problems, is now completely off.
Impression:
- Bioidentical hormone curtail was successful.
- EBV and HP antibody levels appear stable
- We should reassess thyroid autoimmunity now since HP and EBV appear stable.
Recommendations:
- Continue on this program
- – Diet: autoimmune paleo diet/normal paleo diet hybrid based upon reintroduction
- – Hormonal: adrenal adaptogenic herbal blend
- – GI: Lacto/bifido probiotic, digestive bitters
- Through discussion June and decided that we did not need to retest her thyroid antibodies now since she was doing so well and that we would follow up as needed.
Visit 9 (1 year and 3 months later)
- Overall June is still doing well but she wanted to check back in on H. Pylori, EBV and her thyroid autoimmunity.
- June is also now on a lower dose of thyroid Rx, Levothyroxine 75 mcg.
Lab Findings – we asked June to collect these labs before coming into the office.
- AThyroid-Stimulating Hormone (TSH)
- T-4, Free (Thyroxine, Free)
- T-3, Free (Triiodothyronine, Free)
- 0.130-L
- 1.74
- 2.5
- Epstein-Barr Profile (EBV)
- – IgG 198-H, Nuclear IgG >600.0-H, Early Ab IgG 26.8-H *slight improvement*
- Helicobacter pylori Antibodies,
IgA, IgG, IgM - Helicobacter pylori Urea Breath Test
- Thyroid Autoantibodies (TPO and TGA)
- IgG >8.0-H, IgA 20-H,
IgM-normal - Positive Abnormal
- TPO 73-H, Thyroglobulin 310.3-H
Subjective Assessment:
- June has maintained all previous improvements
Impression:
- June is doing great and has even been able to decrease her thyroid Rx dose. In fact she may even be able to decrease her dose further based upon today’s lab findings.
- Her H. Pylori antibodies are essentially unchanged. Her EBV early antigen (EA) has improved slighity, in time and with not treatment.
Recommendations:
- Continue on this program;
- – Diet: autoimmune paleo diet/normal paleo diet hybrid based upon reintroduction
- – Hormonal: adrenal adaptogenic herbal blend
- – GI: Lacto/bifido probiotic, digestive bitters
- June and I discussed trying a protocol of magnesium, selenium, and CoQ10, which had recently been shown to dampen thyroid autoimmunity. We had also decided to treat H. Pylori one more time. We agreed to have her start today on the following:
- – Perform 2 month of H. Pylori treatment; herbal antimicrobials, mastica, and S. boulardii.
- – Start Mg, Se, CoQ10 and stay on this until our follow up
- – Before our next visit perform retesting of H. Pylori and thyroid autoimmunity through LabCorp
Visit 10 (6 months later, from last visit)
June is generally feeling the same, which is very good.
Retesting of H. Pylori and thyroid autoimmunity through LabCorp
- Thyroid-Stimulating Hormone (TSH)
- T-4, Free (Thyroxine, Free)
- Helicobacter pylori Antibodies,
- Helicobacter pylori Urea Breath Test
- Thyroid Autoantibodies (TPO and TGA)
- 0.261- L
- 1.61
- IgA, IgG, IgM – IgG >8.0- H, IgA 20.3-H
- Positive Abnormal
- TPO 76-H, 312-H
Subjective Assessment:
- June has maintained all previous improvements
Impression:
- We reaffirmed June may need less thyroid Rx. She is still on 75 mgc Levo and may even need to decrease her dose again.
- Additional treatment of H. Pylori did not produce any results in her symptoms or her thyroid autoimmunity. H. Pylori is likely functioning as a commensal in June’s microbiota.
- June’s thyroid antibody findings are likely as good as they can get. Regarding TPO antibodies, this level is associated with very minimal risk of progression of hypothyroid. Interpretation of TGab levels are less clear; this level may put her at increased risk for hypothyroid progression, but there is not much else we can treat to improve this. More importantly, the fact that she is needing less thyroid hormone and feeling well is a good prognostic indicator that her thyroid function is improving.
Recommendations:
- Continue on this program
- – Diet: autoimmune paleo diet/normal paleo diet hybrid based upon reintroduction
- – GI: Lacto/bifido probiotic, digestive bitters
- Discontinue Mg, Se, and CoQ10 protocol. Also slowly wean off the adrenal adaptogens.
- Follow up as needed.
Dr. Ruscio’s Comments
June’s case teaches us a lot. It illustrates the power of the gut as June was able to decrease her dose of thyroid hormone as her gut healed. The gut healing likely came from probiotics, digestive bitters, and by reducing the total load of H. Pylori.
It also teaches us that we do not need to treat lab results until they are “normal”. Sometime an “abnormal” finding is perfectly normal. H. Pylori and EBV illustrate this. Most notably the EBV early antigen improved markedly but still remained ‘abnormal/elevated’.
Had this case been handled wrong June would be walking around with “fear of autoimmunity.” She may have very likely been exposed to several rounds of unnecessary treatments trying to force the antibodies lower. Overtreatment of autoimmunity is one the most damaging practice mistakes I see in the field.
June is feeling terrific. Yes she has some “abnormal” lab findings but it’s our job as well-educated clinicians to teach our patients what this actually means. In June’s case it doesn’t mean anything. We reduced her H. Pylori load, viral load, reduced need for medication, and improved all of her symptoms. We now get to do the best thing any clinician can expect to do…. Tell our patients to follow up if or when it’s needed.
I’d like to hear your thoughts or questions regarding any of the above information. Please leave comments or questions below – it might become our next practitioner question of the month.

Like what your reading?
Please share this with a colleague and help us improve functional medicine
Discussion
I care about answering your questions and sharing my knowledge with you. Leave a comment or connect with me on social media asking any health question you may have and I just might incorporate it into our next listener questions podcast episode just for you!