Practitioner Research Review – April 2019
Dr. Michael Ruscio’s Monthly – Future of Functional Medicine Review Clinical Newsletter
Practical Solutions for Practitioners
In Today’s Issue
Research
- Dr. Rusico’s Comparison of Two Popular DNA-based Stool Tests
- Secretome of Intestinal Bacilli: A Natural Guard against Pathologies
- Why Is Working Memory Performance Unstable? A Review of 21 Factors
- Rapid-Fire Research – ultra-concise summaries of noteworthy studies
- Guidelines for the investigation of chronic diarrhea in adults: British Society of Gastroenterology, 3rd edition
![]()
Research
*Please note: the case study and research studies are not meant to be mutually reinforcing. There is often concept overlap, however the research studies are a collection of the most clinically meaningful research that has been published recently.
Dr. Rusico’s Comparison of Two Popular DNA-based Stool Tests
Study Purpose
- To compare the cost and markers of two popular DNA-based stool tests
- And to compare more traditional culture stool testing to DNA testing
Intervention:
- Informal review
- What tests are being compared
- Diagnostic Solutions Laboratory (DSL): GI-Map stool test
- Cost: patient cash $359, list $544
- This is a DNA test using PCR (specifically, RT-PCR aka qPCR).
- Doctor’s Data: GI Pathogen Profile, multiplex PCR
- Cost: prepaid/billed to office $299, regular price $479
- Their DNA/PCR stool test.
- And their stool culture aka MALDI-TOF MS stool test (a bit more of your traditional stool test).
- The Comprehensive Stool Analysis / Parasitology x3 – Cost: $394
- or the curtailed version of Comprehensive Parasitology x3 – Cost: $259
- Diagnostic Solutions Laboratory (DSL): GI-Map stool test
Main Results:
- This is a contentious issue, there may not be a ‘right’ answer but rather it’s a decision of weighing pros/cons of each test and which testing philosophy you feel to have the most merit.
DNA Testing Comparison
- The Doctor’s Data DNA test focuses more on assessing the entire GI ecosystem. Regarding the use of culture testing, they feel a culture-based assessment is a more accurate way of measuring pathogens.
- So, Doctor’s Data recommends DNA for assessing ecosystem and culture for assessing pathogens.
- Alternatively, The GI-Map test uses DNA testing with a focus on the detection of pathogens and potential pathogens (aka opportunists). It does not look to assess the ecosystem.
- Who is right? Which approach is best?
- I feel the more viable approach to focus on detecting pathogens/potential pathogens. If you have a healthy diet and lifestyle inputs, you are supporting a healthy ecosystem. The next step is to determine if pathogens are still maintaining their niche and then use antimicrobial therapies to dislodge their foothold and thus allowing the ecosystem to recalibrate to eubiosis. So, I do not feel it prudent to assess and subsequently attempt to manipulate the ecosystem. Rather, focus on creating a healthy host (healthy inputs) and then if they are non-responsive look to identify and treat pathogens.
- See further down my write up for an expansion on this
- This does not mean you should stop using Doctor’s Data. It is Doctor’s Data’s contention that culture-based testing is superior to PCR/DNA for detecting these pathogens, hence they offer their culture-based testing (Comp Para x3 and Comp Stool with Para x3).
- So, we then need to answer the question, whose test is better for detecting pathogens and potential pathogens. DSL’s GI-MAP DNA-based test or Doctor’s Data’s culture-based test.
DNA Versus Culture Testing Comparison
- Again, the real question is, for detection of pathogens and potential pathogens what is the more accurate measure, DNA or a culture-based assessment.
- Some evidence [1] cited by Dr. Gurevich in a recent podcast) has found DNA testing to be more accurate than traditional culture testing, HOWEVER, the details here matter
- The DNA testing used by DSL’s GI-MAP is not the same as used in the research.
- The DSL’s GI-MAP reagents are developed by them and have not been published in peer-reviewed research, so they have not been fully validated. They are using reagents developed in-house.
- DSL’s GI-MAP is using what is thought to be the best method of PCR testing; RT-PCR aka qPCR (real-time or quantitative PCR). But, whether or not this will perform better clinically with their reagents is still yet to be determined.
- Gurevich referenced a study finding PCR was better than culture, HOWEVER, the stool culture testing used in the studies was not the same that Doctor’s Data uses. Doctor’s Data are purportedly also using more accurate methodology (the MALDI-TOF MS). [2]
- The DNA testing used by DSL’s GI-MAP is not the same as used in the research.
- Are you starting to see why I don’t rely too heavily on lab testing? Everything sounds great in theory, and every lab says they have the best methods, and hopefully, they do, but proof of these claims is not yet available.
- Also, there does not appear to be any direct comparison of the MALDI-TOF MS culture approach which Doctor’s Data uses to RT-PCR aka qPCR which DSL’s GI-MAP uses. So, which test is better is based upon supposition.
- What does the research say? It seems evenly split.
- Some data suggests the Doctor’s Data (MALDI-TOF MS) stool testing is better than PCR. [3,4]
- But, data also suggest that PCR suffers from false positives. [5,6,7]
- Other studies feel that PCR/DNA can replace traditional stool testing, but again it is cautioned to be mindful that false positives are possible [8]
- With Doctor’s Data culture testing, IMPORTANT NOTE
- You must add pylori to their Comprehensive Stool w Para x3.
- Or if you are ordering the Para x3 you must use a separate kit for just pylori (you add HP via their a la carte option).
My Conclusion:
- Philosophically I feel the data from Doctor’s Data’s PCR testing to be clinically less relevant.
- You can assess for pathogens and potential pathogens via Doctor’s Data Culture testing or via DSL’s GI-MAP DNA/PCR testing.
- Which is most accurate?
- DSL’s GI-MAP
- The test has not been published and has not been validated in peer-reviewed research… So, all results should be interpreted with caution and examined in the context of the patient.
- DNA (DSL’s GI-MAP) testing is more sensitive but may suffer from false positives (lower specificity).
- Their updated version of the PCR testing should be the most accurate to date, but this hasn’t been proven.
- Doctors Data’s
- stool testing (MALDI-TOF MS) may not suffer from false positives and may be able to detect pathogens missed by older PCR tests.
- How this test compares to the new PCR testing has not been assessed.
- Conclusion:
- There is no clear consensus, you can use either.
- Scientifically, the MALDI-TOF culture test has better evidence to support it in a few parasitology studies. [9]
- I currently use both the DSL’s GI-MAP and the Doctor’s Data’s culture test at the same time in severe cases and either one or the either in more mild cases.
- If cost is an issue, I use the Doctor’s Data’s Para x3 + pylori.
- If cost is not an issue, I use either the DSL’s GI-MAP or the Doctor’s Data’s Stool with Para x3 + pylori.
- DSL’s GI-MAP
Interesting Notes:
- When inquiring with Doctor’s Data as to why they do not offer a wider breadth of PCR testing, they replied as follows
- “Clinical Limitations of PCR: PCR-based platforms have significant limitations in the context of clinical medicine, particularly for complementary and integrative medicine (CAM) in a non-acute care setting. CAM-oriented clinicians are interested in global changes in the composition and quantity of gastrointestinal microbiota, even in the absence of enteropathogens. That is because such perturbations can be the cause of changes in colonic metabolism that can be associated with significant symptoms of dysbiosis and various diseases.”
- I don’t agree with this statement, much of the data here are far from conclusive and function more as a ‘red herring’ than informative
- “Culture has been criticized for the limited number of microorganisms that can be grown, compared to the vast number of microorganisms that have been detected using DNA methodologies. That criticism is used to argue that PCR is superior for evaluation of gastrointestinal microbiota. Of course, culturing all gastrointestinal microorganisms is indeed a daunting, if not impossible, task. However, to put things in perspective, it should be noted that when MALDI-TOF MS is coupled with high-complexity microbiology, Doctor’s Data has the capability to identify at least 1,240 bacteria and yeast organisms—and that does not include speciation of the many Lactobacilli or Bifidobacteria species.”
- OK, so with a quality culture method, we can assess many organisms. This is good.
- “In addition, PCR requires reagents for identification of every genus, let alone species. Therefore, a reliable RTD-PCR based evaluation of microorganisms in a stool specimen that is even 1/10th as comprehensive as that of the MALDI-TOF MS culture approach would be absolutely cost prohibitive, if even possible.”
- It is difficult to assess the veracity of this statement.
- “Changes in the balance among the prevalent beneficial, expected, and even commensal bacteria and their metabolic activities are as important as the absence of the relatively minute levels of pathogenic bacteria in many symptomatic patients.”
- I strongly disagree. It is my view if pathogens are present they poison the milieu making it unfavorable for ‘healthy’ bacteria.
- “Some may recall Dr. Leo Galland’s discussions of deficiency dysbiosis. As a clinician, do you want to know as much as possible about the vast array of microorganisms that are present in your patients’ stool specimens, or do you want to simply inquire about a handful of microorganisms?”
- Actually, the later, which are the more clinically relevant organisms (pathogens and opportunists).
- “In essence, PCR-based methods are better suited to address the question “Is it there?” rather than “What is there?” The DDI culture-based proteomic approach is analogous to casting a broad net, versus using a fishing pole to obtain a census of the types of fish that inhabit a pond.”
- I appreciate with DD is trying to do and I like their non-PCR testing. However, I do not agree with their approach here regarding PCR testing.
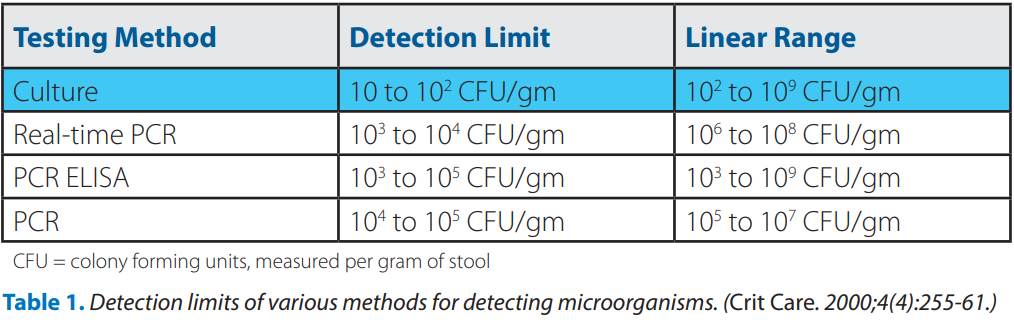
- “The issues of sensitivity and specificity also need to be brought into light in consideration of methods for evaluating gastrointestinal microorganisms. The detection limits of commonly used methods are presented in Table 1. Despite widespread misconception, culture can be 2 to 3 orders of magnitude more sensitive than even RTD-PCR. In fact, culture can reveal the presence of just 1 CFU/g for an enteric pathogen when an enrichment broth is included. PCR-based methods can be less sensitive in part due to a high noise-to-signal ratio obtained when rDNA primers try to find mates among a sea of DNA from a fecal specimen.”
- The jury is out on this statement since there is currently no comparison between the DSL’s GI-MAP DNA method to the Doctor’s Data’s MALDI-TOF MS culture method.
- “Further, clinical specificity with respect to microbial identification can be problematic, because the probes used often cannot differentiate closely related microorganisms that have highly conserved sequences of 16S rDNA. PCR-based methods can also be associated with inferior clinical specificity due to the use of inappropriate primers, as well as errors introduced during the amplification process.”
- This is true, in my opinion, as PCR testing can suffer from false positives

- This is true, in my opinion, as PCR testing can suffer from false positives
- “Clinical Limitations of PCR: PCR-based platforms have significant limitations in the context of clinical medicine, particularly for complementary and integrative medicine (CAM) in a non-acute care setting. CAM-oriented clinicians are interested in global changes in the composition and quantity of gastrointestinal microbiota, even in the absence of enteropathogens. That is because such perturbations can be the cause of changes in colonic metabolism that can be associated with significant symptoms of dysbiosis and various diseases.”
Clinical Takeaways:
- You can use either the DSL’s GI-MAP or Doctor’s Data’s culture testing (Comp. Stool w/ Para x3, or Para x3), but for either you must add pylori.
- No consensus has been reached regarding which of these competing functional medicine labs has a better test.
- If using GI-Map, be suspicious of false positive if a result doesn’t fit the clinical context
- If using Doctors Data culture, positive are more likely to be true positives
Dr. Ruscio Comments
- Whew, a lot here. Fortunately, after all that heavy lifting I arrived back at my prior conclusion from before fact-checking… You can use either test. But at least know we can all use either test in confidence and not get swept into the influence of marketing and popularity.
Secretome of Intestinal Bacilli: A Natural Guard against Pathologies
https://www.ncbi.nlm.nih.gov/pubmed/28919884
Study purpose
- This review aims to characterize the Bacillus and Lactobacillus in GIT, as well as the functional roles of the components released by these members of microbial intestinal community. Complex of their secreted compounds is referred by us as the “bacillary secretome.”
Intervention:
- Review, non-systematic
Main Results:
- Bacillus, aka soil-based organisms, appear to be more of a colonizing category of bacteria. Note: this does not mean that they are better as a treatment, it’s important not to conflate a physiological observation with therapeutic efficacy.
- Bacillus spp. as soil microorganisms were considered transient. Recent studies show that they are present in the GIT in the amounts significantly higher than what can be explained by their ingestion with food only. Bacillus spp.(B. pumilus, B. licheniformis, B. clausii, B. subtilis, B. megaterium, B. mediterraneensis, B. thuringiensis) have been isolated from the healthy human GIT, where they are well-adapted and are more colonizing than transient. [10,11,12]
- Again, Bacillus appears to colonize
- Bacilli introduced into the GIT through the consumption of fermented food do integrate the resident microbiome. [13]
- Lactobacilli, while important, only represent a minority of the GI microbiota and most are transient.
- Lactobacilli are historically considered as integral part of human intestinal microbiota. Today, a large body of evidence indicates that only a small number of Lactobacillus species are true autochthonous inhabitants of the mammalian intestinal tract and that most lactobacilli present are allochthonous members derived from food or oral cavity. [14,15]
- Populations of Lactobacillus and Bacillus are constantly in flux. These details may not be as important as how these populations impact the individual.
- Thus, it can be concluded that GIT microbiota including Bacillus and Lactobacillus species undergoes constant dynamic change. In our opinion, distinguishing between the resident and transient intestinal inhabitants is less relevant issue compared to the study of molecular pool released by them.
- Probiotic administration favorably impacts the microbiota, barrier function, motility, and infection.
- The administration of probiotics has been shown to favorably alter the intestinal microbiota balance, enhance intestinal integrity and motility, inhibit the growth of harmful bacteria and increase resistance to infections. [16]
- As I’ve said repeatedly, it’s not that probiotics colonize you per se, rather they help to nudge the ecosystem in a healthier direction.
- For example, consumption of B. coagulans was shown to increase beneficial groups of bacteria in the gut of 65–80 years old humans and production of anti-inflammatory cytokines. [17]
- “ subtilis also retained gut barrier integrity, decreased the endotoxin concentration and reduced gut inflammation” [18,19]
- Host immune function is an important factor affecting the microbiota
- Gut microbiota is regulated by the host through production of non-specific antimicrobial peptides such as defensins (Nakamura et al., 2016), secreted IgA which provides the selection and the maintenance of the commensal bacteria (Fransen et al., 2015), and miRNAs specifically regulating bacterial transcripts and affecting bacterial growth (Liu and Weiner, 2016). [20,21,22]
- Probiotics reduce inflammation. Note: likely through immune system tuning.
- It is the known that probiotics affect key signaling pathways, such as NFκB and MAPK, through pattern-recognition receptors (TLR, NOD) (Bermudez-Brito et al., 2012) enhancing the production of anti-inflammatory cytokines (Nyangale et al., 2015) and reducing the emergence of proinflammatory ones (Selvam et al., 2009). [23,24,25]
Additional Results:
- Stress is an important input affecting the microbiota
- It was demonstrated that the psychological and physical stress of a host affects its gut microbiota and, in turn, gut microflora can modulate host’s mood and appetite. [26]
- Genetics also play a role. Note: this could be why some patients require more treatment than others.
- It was proved that host genetic background affects the composition and function of the gut microbiota, altering the production of microbial metabolites and intestinal inflammation. [27]
- Poor Lactobacillus colonization may increase the risk of bacterial vaginosis
Authors Conclusion:
- “Lactobacilli are well-represented in the human GIT and secrete a number of compounds which have direct and indirect effects on the health of GIT and organism as a whole. Species of Bacillus genus are much less abundant but are capable of producing several times more extracellular molecules than lactobacilli.”
Interesting Notes:
- Despite their minor proportion in the microbiome composition, these bacteria can significantly affect both the intestinal microbiota and the entire body thanks to a wide range of secreted compounds
- The human gut microbiota consists of about 1500 microbial species
- Lactobacillus and Enterobacter dominate the SI
- The majority of the intestinal bacteria produce spores and are transient.
- Healthy gut microbiota can be defined by the presence of the various microbial species that enhance metabolism, resistance to infection and inflammation, prevention against cancer and autoimmunity.
Clinical Takeaways:
- Most probiotics do not colonize the host, but rather are transient.
- However, probiotics do show multiple favorable effects, including improving the health of the microbiota, improved barrier function, reduced inflammation and combating infection.
- Bacillus species are a major player in the gut, many are part of the resident microbiota, and might be able to colonize the host.
- Bacillus are more prevalent than Lactobacillus.
Dr. Ruscio Comments
Many of us are likely privy to the fact that soil-based, or spore-forming, Bacillus species are an important category of probiotics. This paper provides a nice overview of this issue.
Remember, we should not rush to conclude Bacillus are any better due to these observations. We should include them in our probiotic protocols, but always keep an eye on what the evolving body of clinical/interventional research shows.
Why Is Working Memory Performance Unstable? A Review of 21 Factors
https://www.ncbi.nlm.nih.gov/pubmed/29899806
Study purpose
- To assess the impact of various factors known to impact working memory (WM)
Intervention:
- Review, non-systematic
Background:
- Contextual notes: “Working memory (WM) is an individual’s capacity to simultaneously manipulate some information while maintaining other information.” It is my opinion that optimizing WM will lead to faster progress in clinical and entrepreneurial pursuits, as it enhances problem-solving and the ability to make important connections among multiple pieces of data.
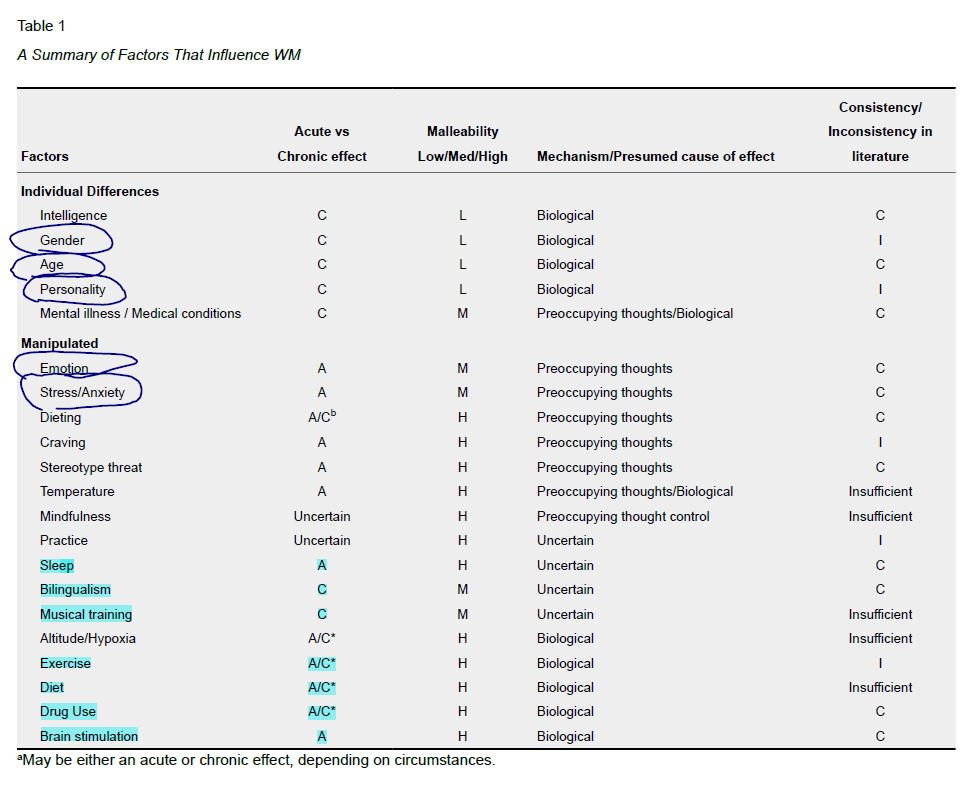
- “The first dimension, and the one that provides the framework for this paper divide factors into two groups: individual differences factors and manipulated (or environmental) factors. Manipulated factors are more malleable, often temporary or reversible in nature, and are generally ones that can be randomly assigned to a person or obtained through some intervention.”
- Table 1 provides a breakdown of the individual (static) and manipulated (amenable) factors associated with working memory

- Most psychologists are in agreement that WM and general intelligence (g) are highly related but separate constructs. [34,35,36]
- WM has been specifically associated with fluid intelligence (gF; novel problem solving) and not crystallized intelligence (gC; verbal and learned experience). [37,38,39,40]
Main Results
SUPPLEMENTS
- Caffeine positively influences WM, especially in extroverts. Even in habitual drinkers.
- Researchers have reported a positive effect of caffeine on WM performance (see Psychoactive Substances section of this paper), and this effect may be particularly strong for extroverts. [41]
- Indeed, nearly every study conducted on caffeine has found increased attention and WM as a result of consumption, with few exceptions (e.g. Smith, Clark, & Gallagher, 1999). [42]
- Even habitual caffeine consumers still show increased WM performance after caffeine consumption. [43]
- 200 mg may be a dose ceiling beyond which no additional results are garnered
- conclude that 200mg of caffeine is optimal for performance on a spatial WM task. Past this amount, the effects do not significantly improve with dosage. [44]
- Ginseng has shown benefit on WM
- Consumption of American ginseng improved WM performance on the Corsi block test at one, three, and six hours post administration. [45]
- As have Ginseng plus Gingko
- found improved WM in a 14-week double blind study of 256 people taking both 60mg Gingko biloba and 100mg ginseng. Gingko and ginseng improved both spatial and verbal WM compared to baseline and the placebo group, although spatial WM saw greater increases, within hours of administration and over the fourteen weeks the study was conducted. [46]
OTHER INTERVENTIONS
- A positive mood favorably effects working memory and vice versa for a negative mood
- In general, negative emotion seems to have an impairing effect on WM; however, under certain circumstances, positive emotion and motivation can enhance WM performance (Table 1).
- Anxiety has a negative effect on WM
- Anxiety has a uniformly detrimental effect on WM performance, and the root of this effect is the use of attentional resources by preoccupying thoughts centered on the anxiety-producing stimulus. The effect of stress and anxiety on WM performance is generally acute, and there is a medium amount of malleability (Table 1).
- Diets which lead to high levels of cravings (what I would term a partially unhealthy diet) lead to reduced working memory
- The effects of dieting may be both acute and chronic, with a high degree of malleability (Table 1). Similar to anxiety, the act of dieting seems to impair WM performance by consuming attentional resources through preoccupying thoughts.
- Prolonged cold temperature might have a negative impact, but data are unclear
- The existing literature suggests cold temperatures negatively influence WM performance. The mechanism of this relationship might be stress and is certainly related to levels of catecholamines in the brain. In Table 1, we describe temperature as an acute, highly malleable manipulated factor; however, the research in this area is sparse and too many questions remain for a firm conclusion as to the nature of this factor.
- The effect of mindfulness/meditation is unclear
- Because few studies have been conducted in this area and because of uncertainty regarding the duration of effect (Table 1), we cannot make firm conclusions about the effect of mindfulness on WM at this time.
- Sleep deprivation has a negative effect
- We view sleep as having an acute and highly malleable effect on WM performance, although the exact mechanism of the effect is uncertain (Table 1).
- Learning a second language has a positive impact
- Regardless of the role individual WM components play, it seems clear that WM is closely related to learning a second language.
- Playing a musical instrument has a positive impact. However, it is also possible that selection-biased exists and those who have higher WM are drawn toward musical training. This same holds for bilingualism
- Both children and adults who have received music training outperform non-musicians on various measures of WM, both verbal and spatial. [47,48,49]
- Unfortunately, the studies conducted thus far used convenience samples of people who have already received musical training. Similar to bilingualism, this is a potential problem of self-selection: individuals with higher WM may be naturally drawn to music or are more persistent in practicing an instrument. A longitudinal study, with a true experimental design, is needed to address this issue.
- As with bilingualism, the effect of musical training on WM performance is chronic and somewhat malleable due to the effort required for musical success (Table 1).
- Exercise’s impact is mixed and undetermined
- Given the wide variety of results, additional research on exercise and WM is needed and both the timing of the WM test and baseline fitness should be considered.
- Low blood sugar impairs WM, children may be less sensitive to glucose deprivation. Overall, data here are limited and the effect of protein and fat are unclear.
- Conversely, induced acute hypoglycemia can cause impaired WM performance on span tests. [50]
- Some researchers maintain that the effect of glucose is age dependent; that is, younger people need less glucose to see an effect on WM performance. [51]
- Though we label diet as biological in cause and highly malleable (Table 1), the existing literature is too small to make firm conclusions about the effect of diet on WM performance at this time.
- Electrical stimulation has shown benefit also. I am currently looking into a home device for this, stand by…
- The two main forms of stimulation that have been investigated are transcranial direct current stimulation (tDCS) and repeated transcranial magnetic stimulation (rTMS).
- based on this meta-analysis, they conclude that rTMS of the dlPFC significantly improves WM performance. Although tDCS significantly improved reaction time, it did not influence the accuracy. [52]
Limitations:
- This was not an exhaustive review.
Authors Conclusion:
- na
Clinical Takeaways:
- Caffeine, gingko, and ginseng can all improve working memory
- Mood and sleep impact WM
- Bilingualism and musical training improve WM
- Electrical stimulations improve WM
Dr. Ruscio Comments
This paper just scratches the surface of a burgeoning field of research. Look for more on this topic in the future as I pull on this string.
Rapid-Fire Research: Ultra-Concise Summaries of Noteworthy Studies
Guidelines for the investigation of chronic diarrhoea in adults: British Society of Gastroenterology, 3rd edition.
https://www.ncbi.nlm.nih.gov/pubmed/29653941
- Below are taking from this paper
- Chronic diarrhea is defined as “the persistent alteration from the norm with stool consistency between types 5 and 7 on Bristol stool chart and increased frequency greater than 4 weeks duration,” where Bristol 5 is soft blobs with clear-cut edges passed easily and Bristol 7 is entirely liquid.
- Here are the key recommendations for the evaluation of adults with chronic diarrhea:
- (1) Perform a detailed history and physical, and order a complete blood count (followed by ferritin if anemic), a thyroid-stimulating hormone test, and serology for celiac disease (tissue transglutaminase or antiendomysium).
- (2) Test stool for Clostridium difficile, ova and parasites, and calprotectin (abnormal inflammatory bowel disease), and consider a fecal immunochemical test.
- (3) In patients with altered bowel habits, rule out colorectal cancer with a colonoscopy. In patients without frank rectal bleeding, order fecal immunochemical testing to exclude cancer.
- (4) If symptoms persist, refer for further investigation.
- (5) Further testing could include a hydrogen breath test for lactose intolerance, video capsule endoscopy, fecal elastase testing for fat malabsorption, tests for bile acid diarrhea, and magnetic resonance imaging for the evaluation of chronic pancreatitis.
- The authors of the guideline advocate early testing for celiac disease, which may be more appropriate in a referral population and in the United Kingdom where the blood test is likely less expensive; its use as a screening test or in a low prevalence population would have a low positive predictive value.
- Dr. Ruscio’s notes
- This overview is helpful for clinicians; however, practice guidelines might be changing in light of Pimentel’s development of an IBS-diagnosing test, IBS Smart. Note, this is the next generation of the prior versions of this test; IBS Detex and IBS Check. This test assesses the underlying cause of some IBS, autoimmunity (CdtB and vinculin). The utility of this test is it can rule out more invasive testing for the causes of diarrhea, like celiac and IBD screening. We will be releasing an interview with Dr. Pimentel on this soon.
I’d like to hear your thoughts or questions regarding any of the above information. Please leave comments or questions below – it might become our next practitioner question of the month.

Like what your reading?
Please share this with a colleague and help us improve functional medicine
Discussion
I care about answering your questions and sharing my knowledge with you. Leave a comment or connect with me on social media asking any health question you may have and I just might incorporate it into our next listener questions podcast episode just for you!